| B-complex vitamins act as coenzymes in many metabolic pathways
|
| With the exception of vitamin B12 there is no storage capacity for water-soluble vitamins. As a consequence of the absence of storage, all water-soluble vitamins must be regularly supplied as constituents of the diet. Any excess of these vitamins is excreted in the urine. In contrast to the fat-soluble vitamins there is no common toxicity associated with excess of these vitamins.
|
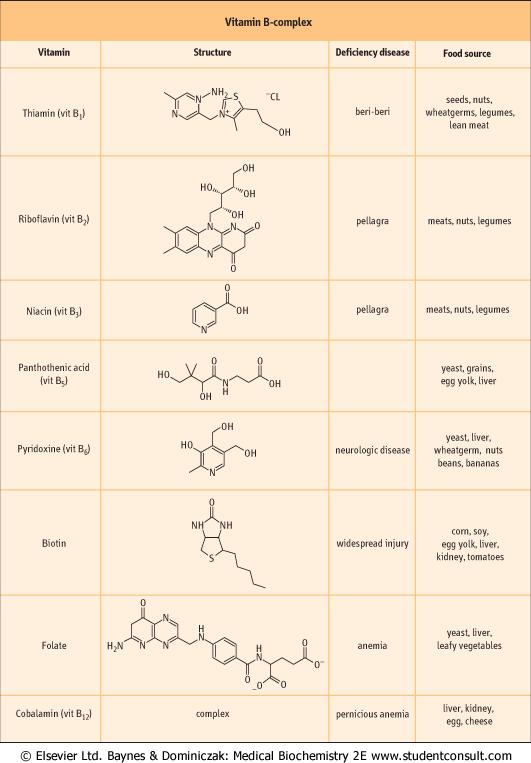
| B-complex vitamins are essential to the normal metabolism of all cells and are involved as coenzymes in many reactions. The B vitamins and their deficiency states are listed in Figure 10.6. Patients often present with multiple deficiencies: a deficiency of a single B vitamin is rare.
|
| Thiamin is essential for carboxylation reactions
|
| Thiamin, in its active form as thiamin pyrophosphate, is essential for carboxylation and some reactions catalyzed by transferases, and for normal carbohydrate energy metabolism (see Chapter 8). Thiamin is required for the transketolase reaction in the hexose monophosphate pathway (see Chapter 11). Although the pathways which require thiamin are well characterized, their failure in deficiency states and the signs and symptoms of deficiency are not clearly related.
|
| Thiamin deficiency is associated with alcoholism
|
| Loss of appetite, constipation, and nausea are early symptoms of thiamin deficiency, progressing to depression, peripheral neuropathy, and unsteadiness, the latter related to impaired nerve cell function. Further deterioration in thiamin status results in mental confusion (loss of short-term memory), ataxia and loss of eye coordination. This combination, often seen in alcoholic patients, is termed Wernicke-Korsakoff psychosis. Severe thiamin deficiency results in beri-beri, either 'dry' (without fluid retention), or 'wet' (associated with cardiac failure with edema). Beri-beri is characterized primarily by advanced neuromuscular symptoms, and occurs in populations relying exclusively on polished rice for food. Wet beri-beri is particularly associated with alcoholism. The signs and symptoms of deficiency may be also seen in the elderly or in low-income groups with poor diet. The measurement of erythrocyte transketolase activity is the most frequently used test to assess thiamin status. Recently is has also been measured by high-pressure liquid chromatography (HPLC).
|
| The greater the caloric intake, the larger the requirement for B vitamins
|
| Diseases that are associated with high caloric requirement require greater intake of thiamin and other B vitamins. Importantly, increased energy supply, in particular from carbohydrates, requires increased amounts of B vitamins as to cope with the increased enzyme activity. Therefore, beriberi might develop on a high-carbohydrate diet.
|
| Riboflavin is associated with oxidoreductases
|
| Riboflavin is attached to the sugar alcohol, ribitol. The molecule is colored, fluorescent, decomposes in visible light but is heat-stable. It is found in the oxidoreductases as flavin mononucleotide (FMN) and flavin adenine dinucleotide (FAD), and is required for the energy metabolism of both sugars and lipids (see Chapter 8). The activation of riboflavin is via an ATP-dependent enzyme system resulting in the production of FMN and FAD.
|
| Lack of riboflavin in the diet causes a generally nonfatal deficiency syndrome of inflammation of the corners of the mouth (angular stomatitis), the tongue (glossitis) and scaly dermatitis. A degree of photophobia may also exist. Owing to its light sensitivity, riboflavin deficiency may occur in newborn infants with jaundice, who are treated by phototherapy. Hypothyroidism is also known to affect the conversion of riboflavin to FMN and flavin adenine FAD. The measurements of erythrocyte glutathione reductase activity are used to determine the riboflavin status.
|
| Niacin is required for NAD+ and NADP+ synthesis
|
| Niacin is a generic name for nicotinic acid or nicotinamide, either of which is an essential nutrient.
|
| page 133 |  | | page 134 |
| Figure 10.6 Structure, sources and deficiency diseases of B vitamins (see also Fig. 13.6). |
| page 134 | | | page 135 |
Niacin is active as part of the coenzyme nicotinamide adenine dinucleotide (NAD+) or nicotinamide adenine dinucleotide phosphate (NADP+) which participate in in oxidoreductase reactions. The active form of the vitamin required for synthesis of NAD+ or NADP+ is nicotinate, and therefore nicotinamide must be deamidated before becoming available for synthesis of these coenzymes. Niacin can be synthesized from tryptophan and hence, in the truest sense, is not a vitamin. The conversion is, however, very inefficient and
cannot supply sufficient amounts of niacin. In addition, the conversion requires thiamin, pyridoxine, and riboflavin, and on marginal diets such a synthesis would be problematic. The requirement for niacin is also related to energy expenditure. can be synthesized from tryptophan and hence, in the truest sense, is not a vitamin. The conversion is, however, very inefficient and
cannot supply sufficient amounts of niacin. In addition, the conversion requires thiamin, pyridoxine, and riboflavin, and on marginal diets such a synthesis would be problematic. The requirement for niacin is also related to energy expenditure.
|
| Severe niacin deficiency produces dermatitis, diarrhea and dementia
|
| Niacin deficiency initially produces a superficial glossitis but may progress to pellagra, which is characterized by dermatitis, sunburn-like skin lesions in areas of body exposed to sunlight and to pressure, diarrhea, and dementia. Untreated pellagra is fatal. Certain drugs, e.g. isoniazid, also predispose to niacin deficiency. In the modern world pellagra is a medical curiosity. Very high doses of niacin can cause hepatotoxicity which is reversible on withdrawal.
|
| Pyridoxine is important in amino acid metabolism
|
| Vitamin B6 is a mixture of pyridoxine, pyridoxal, pyridoxamine, and their 5'-phosphates. Pyridoxine is the major form of vitamin B6 in the diet, and pyridoxal phosphate is the active form of the vitamin. Pyridoxal phosphate participates as a cofactor in amino acid metabolism, and also in the glycogen phosphorylase reaction.
|
| All forms of the vitamin are absorbed from the gut, during which some hydrolysis of the phosphates occurs. Most tissues, however, contain pyridoxal kinase, thus resynthesizing the active phosphorylated forms required for the synthesis, catabolism and interconversion of amino acids (see Chapter 18). Pyridoxine is also required for synthesis of the neurotransmitters, serotonin and noradrenaline (see Chapter 40), for the synthesis of sphingosine, a component of sphingomyelin and sphingolipids (see Chapter 26), and for the synthesis of heme (see Chapter 28).
|
| Vitamin B6 requirements increase with high protein intake
|
| Owing to the central role of vitamin B6 in amino acid metabolism, requirements for this vitamin increase with protein intake. Vitamin B6 deficiency causes irritability, nervousness and depression in its mild form, progressing to peripheral neuropathy, convulsions and coma in severe deficiency. Severe deficiency is also associated with a sideroblastic anemia. The antituberculosis drug, isoniazid, by binding to pyridoxine, and the oral contraceptive pill, by increasing the synthesis of enzymes requiring the vitamin, interfere strongly with pyridoxine and deficiency may occur. Peripheral neuropathy in association with isoniazid is also well recognized. The debate concerning the contraceptive pill continues but it is generally accepted that there is an increased requirement for pyridoxine. As with other B vitamins, assessment of pyridoxine status is based on the measurement of erythrocyte enzymes, in this case, aspartate aminotransferase.
|
|