| METABOLISM AND MUSCLE CONTRACTION
|
| Short-duration, high-intensity contractions
|
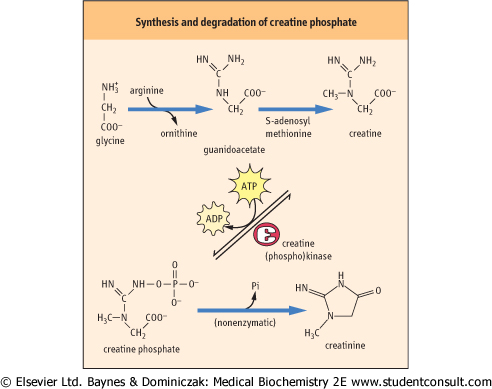
Figure 19.6 Synthesis and degradation of creatine phosphate (creatine-P). Creatine is synthesized from glycine and arginine precursors. Creatine-P is unstable and undergoes slow, spontaneous degradation to Pi and creatinine, the cyclic anhydride form of creatine, which is excreted from the muscle cell into plasma and then into urine. and arginine precursors. Creatine-P is unstable and undergoes slow, spontaneous degradation to Pi and creatinine, the cyclic anhydride form of creatine, which is excreted from the muscle cell into plasma and then into urine. |
| page 268 |  | | page 269 |
| ASSAY OF CREATININE TO ASSESS RENAL FUNCTION AND URINE DILUTION |
| Since creatine phosphate concentration is relatively constant per unit muscle mass, the production of creatinine is relatively constant during the day. Creatinine is eliminated in urine at a relatively constant amount per hour, primarily by glomerular filtration, and to a lesser extent by tubular secretion. Since its concentration in urine varies with the dilution of the urine, levels of metabolites in random urine samples are often normalized to the urinary concentration of creatinine. Otherwise, a 24 h collection would be required to assess daily excretion of a metabolite. Normal creatinine concentration in plasma is about 20-80 mmol/L (0.23-0.90 mg/dL). Increases in plasma creatinine concentration are commonly used as an indicator of renal failure. The albumin/creatinine ratio in a random urine sample, an indicator of protein filtration selectivity of the glomerulus, is used as a measure of the microalbuminuria to assess the progression of diabetic nephropathy. |
| For short bursts of energy, skeletal muscle relies on its ATP stores and an additional reserve of the high-energy storage compound, creatine phosphate (creatine-P), to regenerate ATP rapidly during the first minute as glycogenolysis is activated. Creatine is synthesized from arginine and glycine (Fig. 19.6), and is phosphorylated reversibly to creatine-P by
the enzyme creatine (phospho)kinase (CK or CPK). CK is a dimeric protein and exists as three isozymes: the MM (skeletal muscle), BB (brain) and MB isoforms. The MB isoform is enriched in cardiac tissue.
|
The level of creatine-P in resting muscle is several-fold higher than that of ATP (Table 19.3). Thus, ATP concentration remains relatively constant during the initial stages of exercise. It is replenished not only by the action of CK but also by adenylate kinase (myokinase) as follows:

|
|
Table 19-3.
Changes in energy resources in working muscle. |
| Body_ID: None |
| Changes in energy resources in working muscle |
| Body_ID: T019003.50 |
| Metabolite | Metabolite concentration (mmol/kg dry weight) |
| Body_ID: T019003.100 |
| | resting | 3 minutes | 8 minutes |
| Body_ID: T019003.150 |
| ATP | 27 | 26 | 19 |
| Body_ID: T019003.200 |
| Creatine-P | 78 | 27 | 7 |
| Body_ID: T019003.250 |
| Creatine | 37 | 88 | 115 |
| Body_ID: T019003.300 |
| Lactate | 5 | 8 | 13 |
| Body_ID: T019003.350 |
| Glycogen | 408 | 350 | 282 |
| Body_ID: T019003.400 |
|
| Body_ID: T019003.450 |
Concentrations of energy metabolites in human leg muscle during bicycle exercise. These experiments were conducted during ischemic exercise, which exacerbates the decline in ATP concentration. They illustrate the rapid decline in creatine-P and the increase in lactate from anaerobic glycolysis of muscle glycogen. Data are adapted from Timmons JA et al. J Clin Invest 1998;101:79-85.
|
| During the initial stages of exercise, muscle glycogenolysis, followed by both anaerobic and aerobic glycolysis, is the major source of energy. Calcium entry into muscle leads to formation of a Ca2+-calmodulin complex, which activates phosphorylase kinase, catalyzing the conversion of phosphorylase b to phosphorylase a. AMP also allosterically activates muscle phosphorylase and phosphofructokinase-1, accelerating glycolysis from muscle glycogen.
|
| Low intensity, long duration contractions
|
| Availability and utilization of oxygen in working muscle are the major limitations for maintaining continuous physical activity. At rest or at low-intensities of physical work, oxygen is readily available and the aerobic oxidation of lipid predominates as the main source of ATP synthesis. However, at higher work intensities oxygen availability and utilization can become limiting, and subsequently the work rate of the muscle decreases. One of the main adaptations to regular vigorous physical activity involves increasing muscle mass and oxygenation (perfusion).
|
| During the first 15-30 minutes of exercise, there is a gradual shift from glycogenolysis and aerobic glycolysis to aerobic metabolism of fatty acids. Perhaps this is an evolutionary response to deal with the fact that lactate, produced by glycolysis, is more acidic and less diffusible than CO2. In any case, the glycogen reserves in muscle are sufficient to support the energy needs of muscle during exercise for only about 1 hour. As exercise continues, epinephrine contributes to activation of hepatic gluconeogenesis, providing an exogenous source of glucose for muscle. Lipids gradually become the major source of energy in muscle during long-term exercise. The oxidative metabolism of lipids is supported by increased perfusion and delivery of oxygen.
|
| Long-term muscle performance (stamina) depends on levels of muscle glycogen
|
| page 269 | | | page 270 |
| THE MEASUREMENT OF CARDIAC TROPONINS IS THE PRIMARY TEST TO DIAGNOSE MYOCARDIAL INFARCTION |
| Myocardial infarction (MI) is the result of blockage of blood flow to the heart (see Chapter 17). Tissue damage results in leakage of intracellular enzymes into blood (Fig. 19.7). Among these are glycolytic enzymes, such as LDH (Chapter 11); however, measurements of myoglobin, total plasma CK and CK-MB isozymes are more commonly used for diagnosis and management of MI. Myoglobin is a small protein (17 000 kDa) and rises most rapidly in plasma, within 2 hours following MI. Although it is sensitive, it lacks specificity for heart tissue. It is cleared rapidly by renal filtration and returns to normal within 1 day. Since plasma myoglobin also increases following skeletal muscle trauma, it would not be useful for diagnosis of MI, e.g. following an automobile accident. Total plasma CK and the CK-MB isozyme begin to rise within 3-10 hours following an MI, and reach a peak value of up to 25 times normal after 12-30 hours; they may remain elevated for 3-5 days. Total CK may also increase as a result of skeletal muscle damage but the measurement of CK-MB provides specificity for cardiac damage. |
| Comment. Enzyme-linked immunosorbent assays (ELISA) for the myocardial troponins are now recommended for the diagnosis and management of MI. These assays depend on the presence of unique isoforms of troponin subunits in the adult heart. Tn-T concentration in plasma increases within a few hours after a heart attack, peaks at up to 300 times normal plasma concentration, and may remain elevated for 1-2 weeks. An assay for a specific isoform in an adult heart, Tn-T2, is essentially 100% sensitive for diagnosis of MI and yields fewer than 5% false-positive results. Significant increases in plasma Tn-T are detectable even in patients with unstable angina and transient episodes of ischemia in the heart. Troponins are commonly used as a component of an algorithm to differentiate high-risk from low-risk patients in terms of need for immediate invasive intervention. |
|
| Marathon runners typically 'hit the wall' when muscle glycogen reaches a critically low level. Glycogen is the storage form of glucose in skeletal muscle, and its muscle concentration can be manipulated by diet. Fatigue occurs when the requirement for ATP exceeds its rate of synthesis. For efficient ATP synthesis, there is a continuing requirement for a basal level of glycogen and carbohydrate metabolism in muscle, even when fats are the primary source of muscle energy. Carbohydrate metabolism is important as a source of pyruvate, which is converted to oxaloacetate by the anaplerotic, pyruvate carboxylase reaction. Oxaloacetate is required to maintain the activity of the TCA cycle - for condensation with acetyl CoA derived from fats. Muscle glycogen can be spared and performance time increased during long-term vigorous physical activity by increasing the availability of circulating glucose, either by gluconeogenesis or by carbohydrate ingestion. Increased utilization of fatty acids is an important
training adaptation to regular vigorous physical activity that can also serve to spare glycogen stores (see also Chapter 20).
|
|