| Insulin promotes the anabolic state by channeling the metabolism towards storage of carbohydrate and lipids, and synthesis of protein. Insulin acts on three main target tissues - liver, muscle, and adipose tissue (Fig. 20.2).
|
Plasma glucose concentration acts as a signal that initiates the islet hormonal response concentration acts as a signal that initiates the islet hormonal response
|
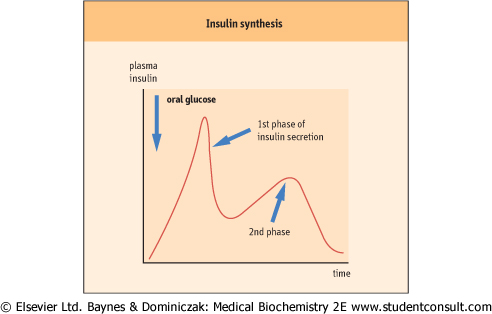
| Glucose stimulates the secretion of insulin and suppresses the secretion of glucagon. Insulin is synthesized in the rough endoplasmic reticulum of the beta cells and is packaged into the secretory vesicles in the Golgi apparatus. Its secretion is initiated by the increased ATP/ADP ratio within the cell, which closes the membrane ATP-sensitive potassium channel. This depolarizes the cell, and the voltage change opens another ion channel: the calcium channel. The entry of calcium ions stimulates the first short phase of insulin secretion (compare this with the neurosecretory granules, Chapter 39) (Fig. 20.2). The second, more prolonged phase requires other signals such as an increase in the concentration of the cytosolic long-chain acetyl-CoA molecules. It also responds to diacylglycerol (DAG) - protein kinase C signaling (see below).
|
| Figure 20.2 Secretion of insulin. Note the biphasic pattern of insulin secretion after glucose load. Glucose is the most important stimulator of insulin secretion. Secretion is also stimulated by some amino acids (branched-chain amino acids - see Chapter 2) and by the stimulation of the vagus nerve. |
| TREATMENT OF DIABETES WITH INSULIN AND TREATMENT OF DIABETIC KETOACIDOSIS |
| Insulin is the mainstay of treatment of type 1 diabetes and is also required in some patients with type 2 where glycemic control cannot be achieved by other drugs. Insulin treatment involves daily subcutaneous insulin injections throughout life. Diabetic patients in whom blood glucose is difficult to control are treated with several injections per day, or sometimes, with a constant insulin infusion, delivered by a programmable, portable pump. The rate of infusion is increased at meal times to help with disposal of exogenous glucose. Diet and exercise are also important in the management of diabetes. |
| Emergency treatment of diabetic ketoacidosis addresses four issues: insulin lack, dehydration, potassium depletion, and acidosis. A ketoacidotic patient requires insulin infusion to reverse the metabolic effect of the excess of anti-insulin hormones, and the infusion of fluids to treat dehydration. Intravenous fluids normally contain potassium supplements to prevent a decrease in plasma potassium hypokalemia. This treatment is usually sufficient to control the metabolic acidosis; however, when the acidosis is severe, infusion of an alkaline solution (sodium bicarbonate) may be required. |
| Type 2 diabetic patients do not usually require insulin treatment because insulin synthesis is at least partly preserved. Instead, the treatment relies on diet and oral hypoglycemic agents. Drugs, such as sulfonylurea derivatives stimulate insulin secretion. Another class of compounds, biguanides (e.g. metformin) reduce hyperglycemia by increasing peripheral glucose uptake. The newest class of drugs are the thiazolidinediones, which also affect the peripheral glucose utilization and improve insulin sensitivity. |
| Insulin signaling involves a membrane receptor, and a multi-step phosphorylation-driven signaling cascades
|
| page 275 |  | | page 276 |
| First, insulin binds to its four-subunit protein membrane receptor on target cells. The β-subunit of the receptor contains a transmembrane protein with an ATP-binding site and has tyrosine kinase activity. The binding of insulin activates the tyrosine kinase, which autophosphorylates the receptor (see Fig. 12.7). Active tyrosine kinase phosphorylates binds other proteins, such as those belonging to the insulin receptor substrate (IRS) family, designated IRS1-4), which are phosphorylated together with other proteins designated Shc, Gab-1 p60dok, APS and Cbl (Cbl is a protooncogene). Subsequently, the IRS protein binds to, and activates, lipid kinase (phosphoinositol kinase) which generates 3' phosphoinositol (PI) phosphates PI -3,4 -P2 and PI-3,4,5-P3; these act as second messengers (see also Chapter 38). They in turn activate the phosphoinositide-dependent protein kinase (PDK1)
which phosphorylates the serine/threonine kinase designated Akt. Finally, Akt participates in insulin-stimulated GLUT4 translocation, a phenomenon underlying cellular glucose uptake. Insulin also stimulates an alternate, PI3-kinase kinase-independent pathway. The response to insulin is also modulated by protein tyrosine phosphatases, enzymes that dephosphorylate the insulin receptor and other molecules in the signaling cascade. (See also Chapter 38.)
|
| Insulin-dependent glucose transport
|
| Insulin-dependent glucose entry into cells is mediated by glucose transporters, in particular GLUT4 which controls glucose uptake into the skeletal muscle and adipocytes. Insulin stimulates exocytosis of GLUT4 molecules to the surface of the cell membrane. Recruitment of the transporter to the plasma membrane requires insulin binding to its receptor and the operation of signaling cascade described above.
|
|