| METABOLISM DURING STRESS, AND THE METABOLIC RESPONSE TO INJURY
|
| page 282 |  | | page 283 |
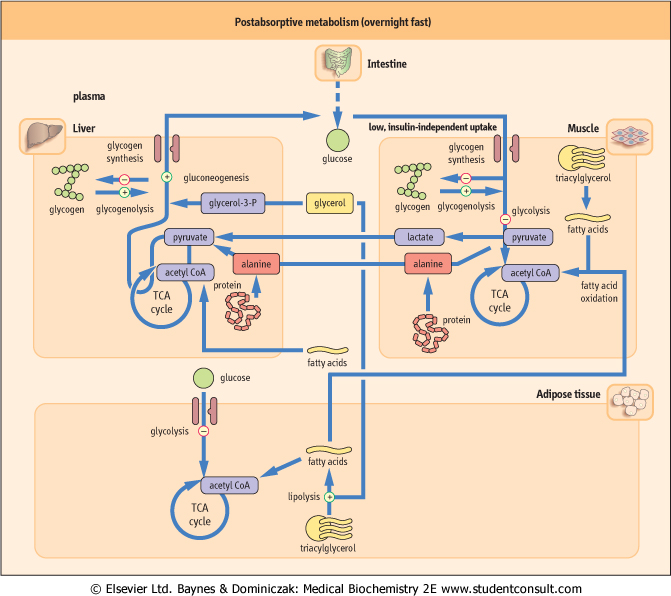
Figure 20.12 Postabsorptive metabolism (overnight fast). In the postabsorptive state, glucose is provided from endogenous sources (glycogenolysis and gluconeogenesis). Alanine and lactate cycles are operative (see Fig. 20.13 for details) There are three main gluconeogenic substrates: alanine, lactate, and glycerol. is provided from endogenous sources (glycogenolysis and gluconeogenesis). Alanine and lactate cycles are operative (see Fig. 20.13 for details) There are three main gluconeogenic substrates: alanine, lactate, and glycerol. |
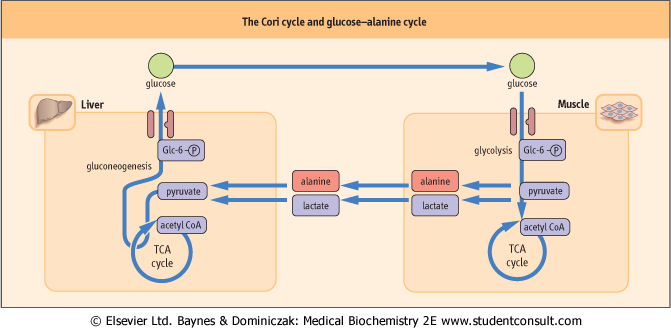
| Figure 20.13 The Cori cycle and glucose-alanine cycle. The Cori (glucose-lactate) cycle allows recycling of lactate back to glucose, but does not contribute to the de novo synthesis of glucose. |
| page 283 | | | page 284 |
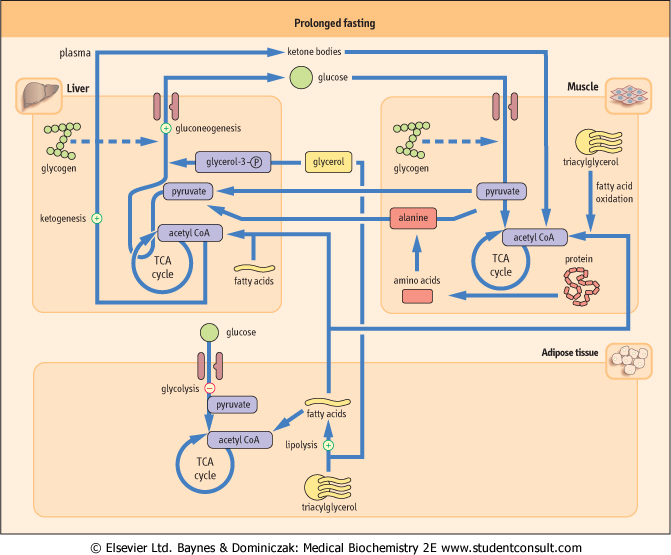
| Figure 20.14 Prolonged fasting. In prolonged fasting, glycogen stores are depleted. The supply of metabolic fuels depends on gluconeogenesis and lipolysis. Ketone bodies become an important energy source; their utilization spares muscle protein. |
| PLASMA GLUCOSE AFTER MYOCARDIAL INFARCTION 245 |
| A 66-year-old woman was admitted to the cardiology ward after suffering a myocardial infarction. Her random plasma glucose level was 10.5 mmol/L (189 mg/dL). The next day a fasting blood glucose was only slightly raised at 6.5 mmol/L (117 mg/dL). Normal fasting plasma glucose is <6.1mmol/L. |
| Comment. This patient underwent a major stress, myocardial infarction, which is associated with a counter-regulatory hormone response and this in turn leads to the elevation of the blood glucose concentration. Care is necessary in the interpretation of raised fasting glucose levels or abnormal glucose tolerance tests in the context of acute illness. |
| Stress is not only 'fight and flight' response but also trauma, injury - particularly burns, surgery, or infection. All are
associated with a metabolic response characterized by hypermetabolism, in which the sympathetic nervous system plays a major role (Fig. 20.15). The main anti-insulin hormones taking part are catecholamines (primarily epinephrine) and glucagon; cortisol is also important.
|
| During stress the brain has priority for fuel supply
|
| page 284 | | | page 285 |
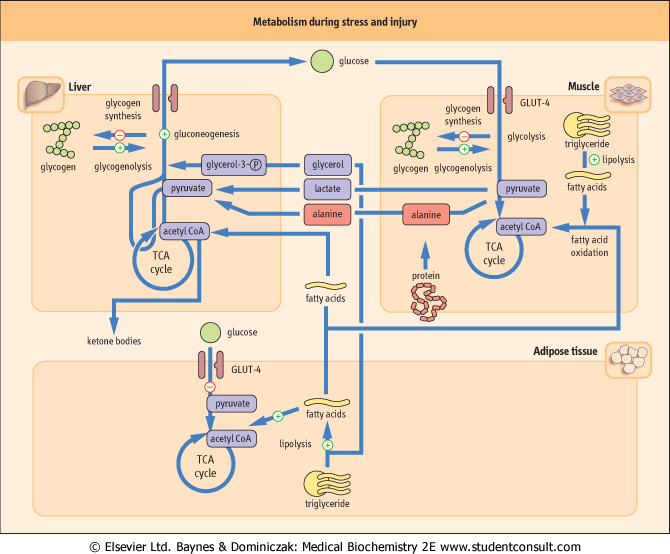
| Figure 20.15 Metabolism during stress and injury. First, glucose is mobilized from all available sources. Epinephrine inhibits the secretion of insulin and the effect of anti-insulin hormones prevails. Stress also induces peripheral insulin resistance. Second, metabolic fuels are provided from fatty acids and from protein catabolism. Such metabolic response occurs in injury, trauma, surgery, burns, and infection. |
| In the first phase of the stress response there is vasoconstriction, which limits blood loss, should it happen. Fuels are then mobilized from all available sources, with provision of glucose for the brain taking priority: high concentrations of epinephrine and glucagon stimulate glycogenolysis and gluconeogenesis to provide endogenous glucose. Decreased peripheral uptake of glucose enhances the hyperglycemic effect. This
results in moderate, frequently detectable, hyperglycemia. Later, the metabolic rate increases and energy is provided primarily from the oxidation of fatty acids and from protein metabolism. Gluconeogenesis from muscle-derived amino acids increases. A negative nitrogen balance is evident approximately 2-3 days post injury.
|
| Stress induces insulin resistance in muscle, adipose tissue, and liver, probably at a postreceptor level
|
| The insulin-dependent transport of glucose in adipose tissue and skeletal muscle decreases most probably because of the suppression of insulin's effect on GLUT-4-mediated glucose uptake. However, at the same time insulin-independent glucose uptake, particularly in muscle, increases. This is caused by tumor necrosis factor (TNF) and other cytokines, such as interleukin-1 (IL-1) (see Chapter 41). TNF also stimulates muscle glycogen breakdown. Glucocorticoids contribute to the stress response by inhibiting glucose transport in peripheral cells. They also facilitate stimulation of gluconeogenesis by glucagon and catecholamines by inducing Glc-6-Pase and PEPCK genes (see Table 20.2). Cytokines, such as IL-6, also affect PEPCK. They stimulate lipolysis in adipose tissue and contribute to muscle proteolysis.
|
| page 285 | | | page 286 |
| MAJOR STRESS ALSO AFFECTS WATER AND ELECTROLYTE METABOLISM |
| A 65-year-old woman underwent a partial gastrectomy. After surgery she was given a standard intravenous fluid replacement. The volume of fluids to be replaced was calculated on the basis of fluid lost in urine, through gastric drainage, and included an allowance for an insensible loss (water loss with breath and sweat). In spite of carefully calculated fluid volume and a normal renal function, the patient developed hyponatraemia due to overload with water. Rapid onset of hyponatraemia may cause convulsions or coma due to cerebral edema. |
| Comment. The response to stress, such as major surgery, includes the stimulation of the secretion of vasopressin (antidiuretic hormone) from the posterior pituitary (see Chapter 35). This causes increased water reabsorption by the kidney and a consequent water retention which needs to be taken into account when prescribing fluid therapy in the postoperative period. (See also Chapters 21 and 22.) |
| There is also an increase in lactate concentration. Lactate is converted to pyruvate in the liver via lactate dehydrogenase. Thus, in the metabolic response to stress there is suppression of anabolic pathways (glycogen synthesis, lipogenesis), increased catabolism (glycogenolysis, lipolysis, and proteolysis), increased insulin-independent peripheral
glucose uptake. All this takes place on the background of insulin resistance. Clinically there is fever, tachycardia (increased heart rate), tachypnea (increased respiratory rate), and leukocytosis (increased number of white blood cells).
|
|