| ASSESSMENT OF FUEL METABOLISM
|
The measurement of plasma glucose is an important clinical test is an important clinical test
|
| The most important laboratory test of fuel metabolism is the simple measurement of plasma glucose. We differentiate between the normal glucose concentration (normoglycemia), too high a level (hyperglycemia), and too low a level (hypoglycemia). Because plasma glucose concentration increases after ingestion of food, it is important to relate the time of blood sampling to the last meal.
|
| The definition of diabetes is based on the evidence that people with glucose levels above the diagnostic level are more likely to develop long-term complications.
|
| Refer to Table 20.5 for the summary of the laboratory diagnosis of diabetes
|
| The fasting plasma glucose is relatively stable. Normal fasting (no caloric intake for approx 10 h) plasma glucose remains below 6.1 mmol/L (<110 mg/dL). A concentration above 6.1 mmol/L but below 7.0 mmol/L (126 mg/dL) is defined as impaired fasting glucose (IFG). The level of 7.0 mmol/L (126 mg/dL) or above, if confirmed, indicates diabetes. Plasma glucose measured irrespective of the meal time (random plasma glucose) is useful for diagnosis of hypoglycemia or severe hyperglycemia, but is of little diagnostic use when the abnormality is mild. The criteria for the diagnosis of diabetes described here are those proposed by the American Diabetic Association in 1997 (see Further Reading).
|
| INSULIN RESISTANCE INCREASES THE RISK OF HEART ATTACK |
| A 45-year-old man was referred to the cardiology outpatient clinic for an investigation of chest discomfort which he felt when climbing steep hills and, in his own words, 'when stressed or excited'. The patient was 170 cm tall and weighed 102 kg (224 lb). His blood pressure was 160/98 mmHg (upper limit of normal = 140/90 mmHg), triglyceride concentration was 4 mmol/L (364 mg/dL) (desirable level <1.7 mmol/L [148 mg/dL]), and fasting plasma glucose was 6.5 mmol/L (117 mg/dL). His resting ECG was normal but an ischemic pattern was observed during exercise. His plasma insulin response to the oral glucose load was higher than normal. |
| Comment. This obese man presented with arterial hypertension, hypertriglyceridemia, and impaired fasting glucose. The impaired fasting of glucose in this case was due to peripheral insulin resistance. Such a cluster of abnormalities is called metabolic syndrome and carries a high risk of coronary heart disease. |
| Oral glucose tolerance test assesses the plasma glucose response to the ingestion of glucose
|
| Blood glucose response to a carbohydrate load is the principle behind the oral glucose tolerance test (OGTT). For a meaningful result it is essential that the test is performed under standard conditions. The patient should attend in the morning, after approximately 10 h fast. To avoid stress-, or exercise-related change in plasma glucose, the patient should sit throughout the test. The test should not be performed during or immediately after an acute illness.
|
| Fasting plasma glucose is measured first. Next, the patient is given a standard quantity of glucose to drink (75 g in 300 mL of water) and glucose is measured again after 30, 60, 90, and 120 min (Fig. 20.11).
|
| Normally, plasma glucose rises to a peak concentration after approximately 60 min and returns to a near-fasting state within 120 min. If it remains above 11.1 mmol/L (200 mg/dL/min) in the 120-min sample the patient has diabetes, even if the fasting blood glucose is normal. If fasting blood glucose is normal but postload glucose is between 6.1 and 7.8 mmol/L (100 mg/dL and 140 mg/dL, respectively), the condition is classified as impaired glucose tolerance (IGT). Individuals with IGT are at an increased risk of developing diabetes in the future. The interpretation of the OGTT is summarized in Table 20.5. For many years OGTT used to be regarded as a reference test for the diagnosis of diabetes but current evidence suggests that the simpler measurement of fasting plasma glucose is equally accurate.
|
| page 294 |  | | page 295 |
| Urine glucose is an insensitive indicator of glycemic control
|
| At normal plasma concentration, all the glucose filtered through the renal glomeruli is reabsorbed in the proximal tubule, and none appears in the urine (Chapter 22). The urinary threshold for glucose is approximately 10.0 mmol/L (180 mg/dL). At plasma glucose concentrations higher than that, the capacity of the renal tubular transport system is exceeded, and glucose filters into the urine (glucosuria). Rarely, in a patient with the renal glucose threshold lower than normal, glucosuria can be detected at non-diabetic blood glucose levels. Thus, the measurement of urine glucose is not a sensitive test for diabetes.
|
| Testing for the presence of ketones in urine (ketonuria) is clinically important
|
| A high concentration of ketones in urine signifies a high rate of lipolysis. This may occur in healthy individuals during prolonged fasting or on a high-fat diet (see box in Chapter 17). In a diabetic patient, however, ketonuria is a sign of metabolic decompensation which should not be ignored.
|
| Increased plasma lactate indicates inadequate oxygenation
|
| HBA1C IDENTIFIES PATIENTS WHO DO NOT COMPLY WITH TREATMENT OF DIABETES |
| A 15-year-old insulin-dependent boy visited a Diabetic Clinic for a routine check-up. He told the doctor that he complied with all the dietary advice and never misses insulin. Although his random blood glucose was 6 mmol/L (108 mg/dL), HbA1c concentration was 11% (normal 4-6%). He had no glycosuria or ketones in his urine. |
| Comment. Blood and urine glucose results indicate good control of this boy's diabetes at the time of measurement, whereas the HbA1c level suggests poor control over the last 3-6 weeks. The probability is that he only complied with treatment days before he was due to come to the clinic. This is not uncommon in adolescents, who find it hard to accept the necessity to adjust their lifestyle to the requirements of diabetes treatment. |
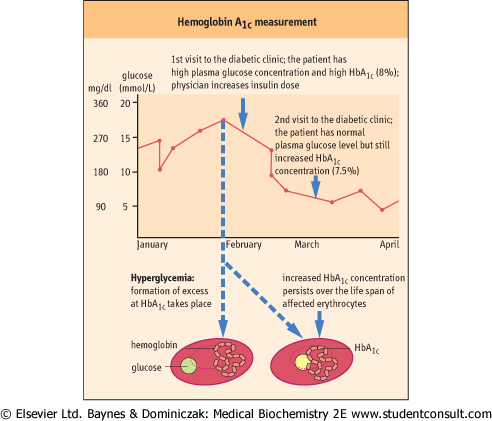
| Figure 20.22 Hemoglobin A1c measurement assesses time-averaged control of glycemia. The concentration of HbA1c in blood reflects time-averaged glycemia over the 3-6 weeks preceding its measurement. To obtain glucose concentrations in mg/dL, multiply by 18. |
| High plasma lactate level indicates increased anaerobic metabolism, and is usually a marker of inadequate tissue oxygenation (hypoxia; see also Chapter 4). The measurements of
plasma lactate are important in rare instances of hyperglycemic nonketotic coma, a life-threatening condition where very high plasma glucose levels, and extreme dehydration, occur in the absence of ketoacidosis.
|
| Glycated hemoglobin (HbA1c) reflects average glycemic control
|
| page 295 | | | page 296 |
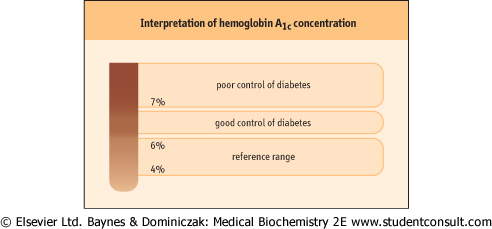
| Figure 20.23 Interpretation of hemoglobin A1c concentration. The HbA1c concentration allows the physician to assess the quality of glycemic control in a diabetic patient. |
| A drawback of the measurement of plasma glucose is that it changes quickly. Therefore, a major advance in the monitoring of diabetic patients has been the measurement of glucose-modified hemoglobin (glycated hemoglobin or HbA1c). Native hemoglobin (HbA) can be converted to a glycated form (HbA1c); such conversion increases during hyperglycemia (Fig. 20.22) and is proportional to the mean plasma glucose concentration. Because the formation of HbA1c at physiologic pH is virtually irreversible, glycation leaves a 'record' of glycemia throughout the rest of the erythrocyte's life: the HbA1c concentration in blood reflects the time-averaged plasma glucose level over the 3-6 weeks preceding the measurement. The normal concentration of HbA1c is 4-6% of total
HbA. Levels below 7% indicate acceptable control of diabetes. Higher levels suggest poor control (Fig. 20.23).
|
| Testing renal function and urinary albumin excretion is important in the assessment of diabetic kidney disease
|
| Urea and creatinine concentrations in the plasma of diabetic patients (see Chapter 21) are routinely tested in diabetic persons. The presence of minimal amounts of albumin present in urine (microalbuminuria, above 200 mg/day) predicts the development of the diabetic nephropathy, and urinary protein excretion (proteinuria) above 300 mg/day is diagnostic for it. To assess microalbuminuria one needs to use a method of measurement which is more sensitive than the conventional method for the measurement of albumin in serum.
|
| When ordering laboratory tests, remember the fast-feed cycle
|
| Blood sampling during the postabsorptive state provides the best assessment of basal metabolism. This is why patients are often asked not to eat anything 8-12 h before having blood taken for laboratory tests.
|
|