| page 321 |  | | page 322 |
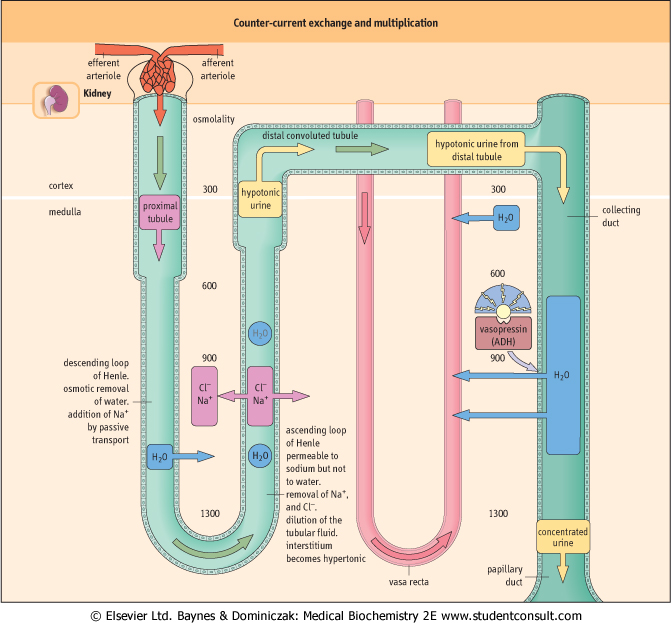
| Figure 22.9 Counter-current exchange and multiplication. The counter-current mechanism is essential for the formation of urine, and for the efficient reabsorption of water in the distal tubule: it enables the kidney to maintain high osmolality in the medulla. The descending and ascending arms of the loop of Henle have different permeability characteristics. In the ascending arm, sodium and chloride ions are pumped out into the interstitial fluid. They then diffuse freely into the lumen of the descending limb, creating a functional 'loop', which perpetuates the increase in osmolality of the filtrate reaching the ascending limb. This is known as counter-current multiplication. |
Figure 22.9 As a result of this, the osmolality of the renal cortex is similar to that of plasma (300 mmol/L), whereas in the medulla it might be as high as 1300 mmol/L. High osmolality of the medulla facilitates reabsorption of water in the collecting ducts. This is known as counter-current exchange. Reabsorbed water diffuses into the medullary blood vessels (vasa recta). The amount of water absorbed is controlled by vasopressin . . |
| Figure 22.9 Counter-current multiplication and counter-current exchange act in concert to enable efficient reabsorption of water in the collecting duct. |
| page 322 | | | page 323 |
| Figure 22.10 Sodium reabsorption in the renal tubules. More than 80% of filtered sodium is actively reabsorbed in the proximal tubule. In addition, sodium and chloride ions are reabsorbed in the ascending limb of the loop of Henle (see also Fig. 22.9). A different mechanism operates in the distal tubule, where sodium reabsorption is stimulated by aldosterone and is coupled with the secretion of hydrogen and potassium ions. Aldosterone causes sodium retention and an increased secretion of potassium. |
| Kidneys excrete from 0.5 L to more than 10 L of urine daily; the average daily volume is 1-2 L. The minimum volume necessary to remove the products of metabolism (mainly
nitrogen excreted as urea) is approximately 0.5 L/24 h. Urine osmolality varies from about 80 to 1200 mmol/L. The osmolality of the glomerular filtrate is about 300 mmol/L, therefore the maximal urine concentration is approximately fourfold. The ability to form concentrated urine in response to fluid deprivation depends on normal tubular function and on the presence of vasopressin.
|
| DIABETES OFTEN LEADS TO THE IMPAIRMENT OF RENAL FUNCTION |
A 37-year-old woman with a 12-year history of type 1 diabetes came for a routine visit to the Diabetic Clinic. She had poor diabetic control and a glycated hemoglobin (HbA1c) value of 8%. Blood pressure was mildly raised at 138/88 mm Hg. A quantitative measurement of albumin in urine revealed protein concentration of 40 mg/L, indicating microalbuminuria. Reference values are:
- HbA1c: desirable value below 6%.
- Microalbuminuria: less than 30 mg/L.
|
| Comment. This patient had mildly impaired renal function and raised blood pressure as a result of glomerular damage from diabetes. The presence of microalbuminuria predicts future overt diabetic nephropathy. Blood pressure should be maintained at <130/80 mmHg preferably with an angiotensin converting enzyme inhibitor drug. |
| Only small amounts of amino acids (0.7 g/24 h), and almost no glucose, are normally present in the urine. Each substance reabsorbed in the renal tubules has its own renal transport maximum (Tmax). Tmax can be exceeded either when the load of a substance becomes too large to handle, swamping the transport system, or when the tubular cells themselves do not function properly. Thus, aminoaciduria may result from an impaired tubular function or from the accumulation
of amino acids such as phenylalanine, leucine, isoleucine, and valine in the plasma.
|
| Analysis of urine (urinalysis) is important in the diagnosis of renal disease, diabetes, and jaundice and helps to diagnose hereditary defects of amino acid transport
|
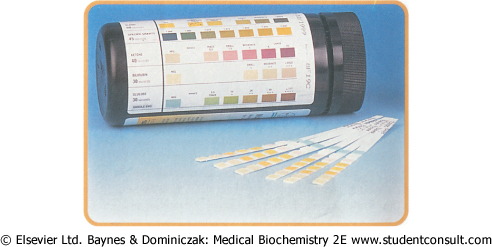
| The analysis of urine carried out in clinical laboratories includes testing for the presence of protein, glucose, ketone bodies, bilirubin, and urobilinogen, and looking for traces of blood. Urinary osmolality is checked to assess the concentrating capacity of the kidney. Specialist investigations include the analysis of urinary amino acids. The urine is also tested for the presence of leukocytes and various crystals and deposits (Fig. 22.11).
|
| page 323 | | | page 324 |
| Figure 22.11 The urine testing (urinalysis) is performed using ready-made dry tests; these are strips coated with reagents immobilized on a plastic support. Dipping the strip in the urine initiates a reaction yielding a colored product. The readout is against a standardized color scale. |
| Protein is normally detectable in the urine in trace amounts only, but this increases significantly when the glomeruli are damaged; the presence of significant amounts of protein in urine is an important sign of renal disease. Even minimal amount of albumin in the urine (microalbuminuria) predicts the development of diabetic nephropathy (see Chapter 20). Larger proteins such as immunoglobulins appear in the urine when the glomerular damage is more extensive: the immunoglobulin light chains (Bence-Jones protein) are present in urine in multiple myeloma (see Chapter 3). In hemolytic anemia, the urine may contain free hemoglobin and urobilinogen. Myoglobin is present in urine in cases of widespread muscle damage (rhabdomyolysis). The measurement of glucose and ketones in the urine, together with their measurements in blood, is important in monitoring the glycemic control (Chapter 20). The measurements
of urobilinogen and bilirubin in urine help to assess liver function (see Chapter 28).
|
|