| Serum creatinine concentration and creatinine clearance
|
| Measurement of serum creatinine is a simple test of renal function that does not require urine collection
|
Administering inulin intravenously to assess the GFR is quite impractical. Instead, we calculate the clearance of creatinine, a compound normally detected in plasma which is derived from phosphocreatine present in skeletal muscles. The clearance of creatinine is similar to that of inulin. There is some tubular reabsorption of creatinine, but this is compensated by an equivalent degree of tubular secretion. To calculate creatinine clearance, one needs a sample of blood, and urine collected over 24 hours. The concentration of creatinine in the serum and the urine is measured. The urine excretion per unit of time is calculated by dividing the total urine volume by the collection time (V, above). The clearance of creatinine is then calculated according to the formula:

|
The concentration of creatinine in serum is 20-80 mmol/L (0.28-0.90 mg/dL). The measurement of serum creatinine is the simplest test of renal function. An increase in serum creatinine concentration is a marker of a decrease in GFR: serum creatinine concentration doubles when the GFR decreases to approximately 50% of its original value. Another test that is used to assess kidney function is the measurement of serum urea . However, because urea is an end product of protein catabolism, its amount in plasma, apart from renal function, is also dependent on factors such as the amount of protein in the diet (Chapter 18) and the rate of tissue breakdown (Fig. 22.12). . However, because urea is an end product of protein catabolism, its amount in plasma, apart from renal function, is also dependent on factors such as the amount of protein in the diet (Chapter 18) and the rate of tissue breakdown (Fig. 22.12).
|
| The newest test to measure renal function is the assessment of cystatin C concentration which seems to provide accurate assessment of moderate decreases in the glomerular filtration rate
|
| Cystatin C is a 122-amino acid, 13 kDa protein belonging to the family of cysteine proteinase inhibitors. It is a product of the 'housekeeping' gene expressed in all nucleated cells, and is produced at a constant rate. Because of its small size and its basic pI, cystatin C is freely filtered through the glomerulus. It is not secreted by the tubules but it is reabsorbed and subsequently catabolized, therefore it does not return to blood. The use of serum cystatin C to estimate GFR follows the same logic as the use of serum creatinine.
|
| page 324 |  | | page 325 |
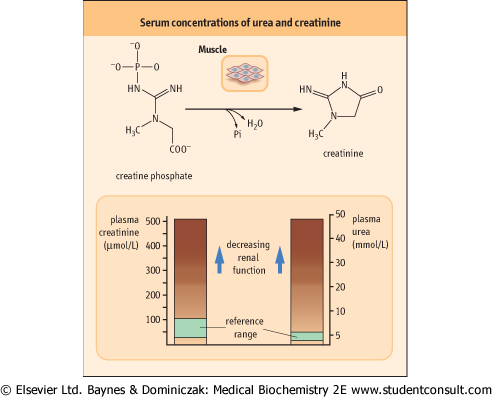
| Figure 22.12 Serum levels of urea and creatinine. The most important biochemical markers of renal function are serum urea and serum creatinine. The upper panel shows the conversion of muscle phosphocreatine into creatinine. Loss of 50% of nephrons results in approximate doubling of serum creatinine concentration. |
| The measurements of serum creatinine and urea concentration are performed as first-line tests and are essential for the diagnosis of renal failure. In renal failure one observes a decrease in urine volume, an increase in serum concentrations
of urea and creatinine, and a decrease in creatinine clearance.
|
|