| Hypercalcemia is most commonly caused by primary hyperparathyroidism and malignancy
|
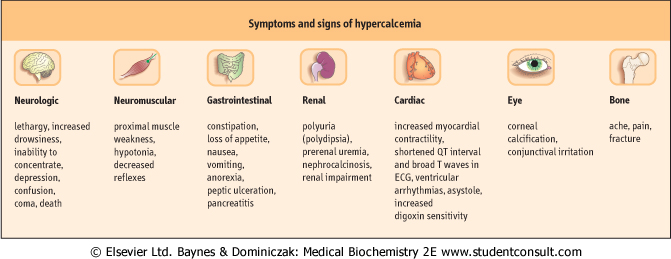
| Figure 24.7 Symptoms and signs of hypercalcemia. Symptoms are more likely as the serum concentration of calcium increases. |
| page 352 |  | | page 353 |
|
Table 24-1.
Common and uncommon causes of hypercalcemia. |
| Body_ID: None |
| Causes of hypocalcemia |
| Body_ID: T024001.50 |
| Common causes | primary hyperparathyroidism
malignant disease
iatrogenic - vitamin D or vitamin D analogs |
| Body_ID: T024001.100 |
| Uncommon causes | thyrotoxicosis multiple
myeloma
sarcoidosis
drug-induced:
thiazide diuretics
lithium
renal failure (acute and chronic)
familial hypocalciuric hypercalcemia |
| Body_ID: T024001.150 |
| PRIMARY HYPERPARATHYROIDISM (HPT) |
| A 52-year-old woman presented to the Accident and Emergency Department of her local hospital with severe right-sided flank pain. Blood was detected on stick testing of urine and radiography revealed the presence of kidney stones. The pain settled with opiate analgesia. Further questioning revealed a history of recent depression, generalized weakness, recurrent indigestion, and aches in both hands. Serum adjusted calcium was 3.20 mmol/L (12.8 mg/dL; normal range 2.2-2.6 mmol/L [8.8-10.4 mg/dL]), serum phosphate 0.65 mmol/L (2.0 mg/dL; normal range 0.7-1.4 mmol/L [2.2-5.6 mg/dL]), and PTH 16.9 pmol/L (169 pg/mL); normal range 1.1-6.9 pmol/L (11-69 pg/mL). |
| Comment. Most patients with primary HPT are now identified when asymptomatic hypercalcemia is discovered on 'routine' biochemical testing or during investigation of nonspecific symptoms. When symptomatic, primary HPT classically affects the skeleton, kidneys, and gastrointestinal tract, resulting in the well-recognized triad of complaints described as: 'bones, stones, and abdominal groans'. Renal stone disease is now the most common presenting complaint. |
| There is a wide individual variation in the development symptoms and signs of hypercalcemia (Fig. 24.7). In general, the higher the adjusted calcium, and the more rapid the increase
in calcium, the more likely are symptoms to be present. In practice, 90% of cases are due to either primary HPT or malignancy; a greater diagnostic challenge is presented when it becomes necessary to differentiate occult malignancy from the less common causes of hypercalcemia (Table 24.1).
|
| Investigation of hypercalcemia
|
| In the majority of cases, the cause of hypercalcemia will be identified by obtaining an accurate history, by clinical examination, and by appropriate biochemical tests. In some cases, however, additional valuable information on causation may be obtained from radiologic investigations and tissue biopsies. The development and ready availability of specific, sensitive, and reliable assays for intact PTH has enabled the clinician to discriminate primary HPT from non-parathyroid causes of hypercalcemia (particularly malignancy): an increased or inappropriately detectable intact PTH in the presence of hypercalcemia is observed in primary HPT, whereas an intact PTH below the limit of detection of the assay (undetectable) is usually observed in non-parathyroid causes of hypercalcemia.
|
| Several laboratory tests may be required to differentiate the various non-parathyroid causes of hypercalcemia
|
In a high percentage of cases, HCM is caused by tumors secreting parathyroid-hormone-related protein (PTHrP). Vitamin D excess or overdose may be obvious from the history, but sometimes only becomes apparent after measurement of the concentrations of vitamins D3 (cholecalciferol), D2 (ergocalciferol ), and 1,25(OH)2D3. Measurement of serum electrolytes, urea, and creatinine will confirm renal failure, and estimation of protein, albumin, and immunoglobulins may indicate the presence of myeloma (Chapter 3), which should be investigated by both serum and urine electrophoresis. Thyroid function tests (measurement of thyroid-stimulating hormone, total thyroxine, and total tri-iodothyronine, or estimation of free thyroid hormone (see Chapter 37) enable diagnosis of thyrotoxic hypercalcemia. Rare causes of hypercalcemia may be diagnosed by estimation of lithium (toxicity or overdose), growth hormone (acromegaly), vitamin A (toxicity), and urine catecholamines (pheochromocytoma, see Chapter 40). ), and 1,25(OH)2D3. Measurement of serum electrolytes, urea, and creatinine will confirm renal failure, and estimation of protein, albumin, and immunoglobulins may indicate the presence of myeloma (Chapter 3), which should be investigated by both serum and urine electrophoresis. Thyroid function tests (measurement of thyroid-stimulating hormone, total thyroxine, and total tri-iodothyronine, or estimation of free thyroid hormone (see Chapter 37) enable diagnosis of thyrotoxic hypercalcemia. Rare causes of hypercalcemia may be diagnosed by estimation of lithium (toxicity or overdose), growth hormone (acromegaly), vitamin A (toxicity), and urine catecholamines (pheochromocytoma, see Chapter 40).
|
| Primary hyperparathyroidism is relatively common
|
| Primary HPT is a relatively common endocrine disease, characterized by hypercalcemia associated with an increased or inappropriate intact PTH. It has an incidence ranging from 1 in 500 to 1 in 1000 of the population. In 80-85% of patients, a solitary parathyroid gland adenoma is present, and the condition is curable by successful removal of the adenoma.
|
| Hypercalcemia associated with malignancy (HCM) is a poor prognostic sign
|
| Hypercalcemia tends to occur late in the course of malignant disease, and is usually a poor prognostic sign. Effective and relatively innocuous treatment for HCM is now available, and can markedly improve the quality of life of these patients, by relieving the symptoms of hypercalcemia.
|
| page 353 | | | page 354 |
| HYPERCALCEMIA ASSOCIATED WITH MALIGNANCY (HCM) |
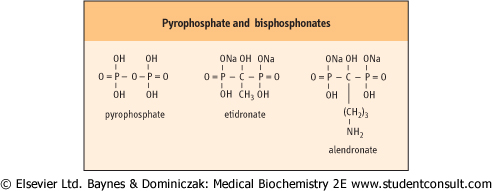
| Treatment of hypercalcemia can greatly improve the quality of life of patients. Symptomatic hypercalcemia or serum calcium concentrations exceeding 3.00 mmol/L (12 mg/dL) would merit treatment. Dehydration results from hypercalcemia-induced polyuria, reduced fluid and food intake, associated vomiting, decreased arginine-vasopressin, AVP (also known as ADH) activity at the distal tubule, and reduced renal perfusion. Fluid replacement corrects hypovolemia and provides a moderate sodium load, which will cause a concomitant increase in calcium excretion. Bisphosphonates (Fig. 24.8) have improved the management of HCM, and are the most effective drugs available for treating hypercalcemia. This group of drugs have their major effects by inhibiting osteoclast activity immediately when infused, and then exert a more prolonged effect by being incorporated into bone matrix in a position normally occupied by pyrophosphate. |
| Calcitonin also inhibits osteoclast activity directly, and decreases renal tubular reabsorption of calcium; downregulation of calcitonin receptors subsequently occurs, and so the calcium-decreasing effect lasts only 4-5 days. |
| Figure 24.8 Structural formulae of pyrophosphate and bisphosphonates. The P-C-P bonds of the biphosphonates can resist enzymic cleavage, and the potency of these drugs is determined by the chemical sequence attached to the carbon molecule. |
| Two major mechanisms of HCM are recognized
|
Calcium reabsorption by the kidney is often enhanced in HCM, interfering with the ability of the kidneys to limit the increased release of serum calcium that results from increased osteoclast activity. There are two main sources of stimulation of the osteoclasts:
- a circulating humoral factor secreted by the tumor;
- a locally active secretory factor(s) produced by the tumor or metastases in bone.
|
| HYPOCALCAEMIA IN THE NEONATE |
| A healthy full-term boy aged 7 days and weighing 3.5 kg was noted by the community midwife to be jittery and feeding poorly at home. On review by the paediatrician, the blood calcium was measured and found to be 1.55 mmol/L. The child responded to calcium supplementation and vitamin D. |
| Comment. Postnatal hypocalcaemia is common, with most levels being above 1.75 mmol/L. In the first thirty-six hours of life, calcium levels fall as the relatively higher maternal levels switch the foetal parathyroid gland off. After 2 days, the concentration increases again. |
| Where a more profound drop in calcium is present, and particularly when it is at the end of the first week of life, other causes may be found. Here the possibilities include primary hypoparathyroidism, maternal hyperparathyroidism with hypercalcaemia, and maternal vitamin D deficiency. Thus, investigations on the neonate and mum are required. |
| Current evidence indicates that the most common cause of HCM is the production, by tumors or their metastases, of a humoral factor, PTHrP (see above), that can circulate in blood and exert its effects on the skeleton and kidneys. Production of PTHrP is common in breast, lung, kidney, or other solid tumors, but is more rare in hematologic, gastrointestinal, and head and neck malignancies. The amino-terminal portion of PTHrP possesses PTH-like activity that results in hypercalcemia, hypophosphatemia, phosphaturia, increased renal calcium reabsorption, and osteoclast activation.
|
| The second type of hypercalcemia is the result of increased bone resorption by osteoclasts stimulated by factors produced by the primary tumor or, more usually, by metastases, that stimulate osteoclasts by alteration of the RANKL/OPG balance. Mediators such as PTHrP, cytokines, and growth factors (e.g. IL-1, TNF-α, lymphotoxin, and TGF-α) have all been shown to possess osteoclast-stimulating activity that results in significant bone resorption. Production of prostaglandins, especially those of the E series (PGE2), has been demonstrated in several classes of tumor, particularly breast cancer. Prostaglandins stimulate osteoclastic bone resorption, and infusion of high concentrations of prostaglandins results in hypercalcemia.
|
| Excess of vitamin D is toxic
|
| Increasing therapeutic use of potent vitamin D analogs, hydroxylated at position 1 or at positions 1 and 25, made vitamin D toxicity the third most common cause of hypercalcemia.
|
|