| Osteoporosis is a common age-related disease of bone
|
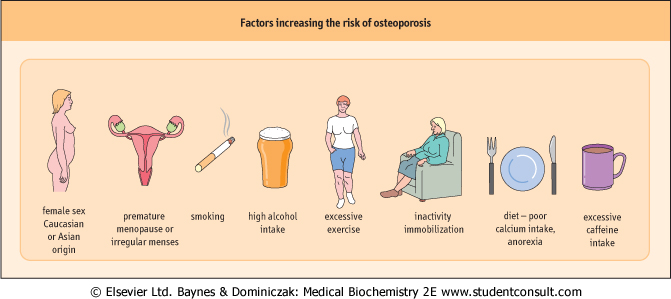
| Osteoporosis can be defined as 'a significant reduction of bone mineral density compared with age- and sex-matched norms, with an increased susceptibility to fractures'. Osteoporosis is associated with aging and, with increasing longevity, a greater percentage of the population will become susceptible to osteoporosis and its sequelae. Bone density decreases from a peak achieved by the age of 30 years in men and women, and the rate of bone loss is accelerated in women after loss of estrogen secretion at the menopause. The progressive loss of bone that takes place with aging is a result of uncoupling of bone turnover over a prolonged period of time, with a relative increase of bone resorption or decrease in bone formation. A number of factors have been recognized as contributing to an increased risk of osteoporosis (Fig. 24.9).
|
| There is much debate on the best therapeutic approach to osteoporosis, and many questions are raised about the possibility of detecting 'fast bone-losers' by measuring biochemical markers of bone metabolism. Most of the available treatments decrease osteoclast activity, and are therefore anti-resorptive, but new therapies are available such as nightly sub-cutaneous injections of PTH(1-34) that have an anabolic action stimulating osteoblast activity and new bone formation.
|
| Paget's disease of bone is a disorder characterized by areas of accelerated bone turnover initiated by increased osteoclast-mediated bone resorption
|
| Osteoclasts in Paget's disease are large, numerous, and multinucleate (up to 100 nuclei); their activity is coupled to increased osteoblast number and activity. A common biochemical abnormality of the disease is increased alkaline phosphatase, which is indicative of increased osteoblast activity. Increased collagen breakdown by osteoclasts results in a high serum and urine concentration of hydroxyproline, pyridinolines, and telopeptides. The bisphosphonates (see Fig. 24.8) have significant antiosteoclastic activity, and are the drugs of first choice for treating Paget's disease.
|
| page 356 |  | | page 357 |
| Figure 24.9 Risk factors and secondary causes of osteoporosis. |
| A 62-year-old woman was admitted to hospital because of sudden onset of severe back pain between the shoulder blades after a fall in her bathroom. Radiography detected a wedge fracture of two thoracic vertebrae reduced bone density. A bone density scan or dual energy X-ray absorptiometry (DEXA) scan showed severely reduced density in femur and spine. She had experienced the menopause after a hysterectomy at age 41 years but had been unable to tolerate hormone replacement therapy (HRT). Biochemical investigations were all within normal limits. |
| Comment. Symptoms of osteoporosis develop at a late stage of the disease, and are often caused by the presence of fracture(s). Hip, vertebral, and wrist fractures are common in patients with osteoporosis, and result in significant mortality and morbidity. HRT can be used to prevent the development of bone loss in postmenopausal women but slightly increases the risk of stroke, heart attack and breast cancer. |
| A 60-year-old woman who had become increasingly infirm and housebound was referred to the Metabolic Outpatient Clinic. She had experienced a gradual onset of diffuse aches and pains throughout her skeleton but especially around the hips. She was having difficulty walking, had generalized weakness, and had recently experienced sudden severe pain in her ribs and pelvis. Radiography detected fractured ribs. Adjusted serum calcium was 2.1 mmol/L (8.4 mg/dL; normal range 2.2-2.6 mmol/L [8.8-10.4 mg/dL]), serum phosphate 0.56 mmol/L (1.7 mg/dL; normal range 0.7-1.4 mmol/L [2.2-4.3 mg/dL]), alkaline phosphatase 300 IU/L (normal range 50-260 IU/L) and PTH 12.6 pmol/L (normal range 1.1-6.9 pmol/L [11-69 pg/mL]). |
| Comment. In severe forms of osteomalacia, biochemical abnormalities are commonly seen, including low serum adjusted calcium, low serum phosphate, increased alkaline phosphatase and increased PTH(1-84). Clinically, patients may have diffuse bone pain or more specific pain related to a fracture, lateral bowing of the lower limbs, and a distinctive waddling gait. Ethnic groups with dark skin are particularly at risk in countries with low-average sunlight, as the majority of vitamin D in the body comes from synthesis by the action of UV light on 7-dehydrocholesterol. This may be exacerbated by traditional dress and a diet that is high in phytates (unleavened bread) and low in calcium and vitamin D. |
| page 357 | | | page 358 |
| The characteristic pathology in osteomalacia is the defective mineralization of osteoid in mature bone. When this occurs in the growing skeleton, there is also loss of maturation and mineralization of the cartilage cells at the growth plate; the
term 'rickets' is used to describe the clinical, radiologic, and pathologic findings seen in children. There are several diverse causes of osteomalacia, many related to abnormalities of vitamin D metabolism.
|
|