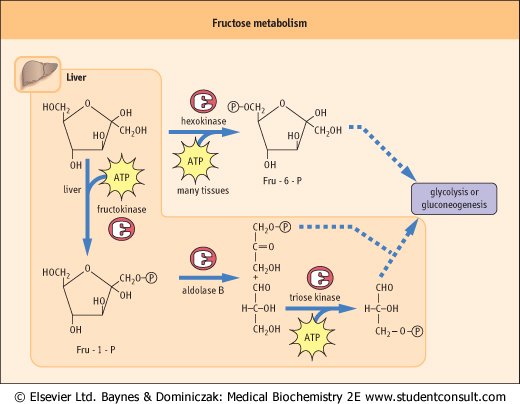
| Figure 25.7 Metabolism of fructose by fructokinase or hexokinase. |
| page 363 |  | | page 364 |
An apparently normal baby began to vomit and develop diarrhea after breast feeding. These problems, together with dehydration, continued for several days, when the baby began to refuse food and developed jaundice, indicative of liver damage, followed by hepatomegaly, and then lens opacification (cataracts). Measurement of glucose in the blood and urine by a specific enzymatic technique indicated that concentrations of glucose were low, consistent with the failure to absorb foods. However, glucose measured by a colorimetric test that determined total reducing sugar indicated that the concentration of sugar was quite high in both blood and urine. The reducing sugar was eventually identified as galactose, indicating an abnormality in galactose metabolism known as galactosemia. This finding was consistent with the observation that, when milk was removed from the diet and replaced with an infant formula containing sucrose rather than lactose, the vomiting and diarrhea stopped, and hepatic function was gradually restored. in the blood and urine by a specific enzymatic technique indicated that concentrations of glucose were low, consistent with the failure to absorb foods. However, glucose measured by a colorimetric test that determined total reducing sugar indicated that the concentration of sugar was quite high in both blood and urine. The reducing sugar was eventually identified as galactose, indicating an abnormality in galactose metabolism known as galactosemia. This finding was consistent with the observation that, when milk was removed from the diet and replaced with an infant formula containing sucrose rather than lactose, the vomiting and diarrhea stopped, and hepatic function was gradually restored. |
| Comment. The accumulation of galactose in the blood is most often a result of a deficiency of Gal-1-P uridyl transferase, which prevents the interconversion of galactose and glucose and leads to the accumulation of galactose and Gal-1-P in tissues. Accumulation of the latter interferes with phosphate and glucose metabolism, leading to widespread tissue damage, organ failure, and mental retardation. In addition, accumulation of galactose in tissues results in galactose conversion via the polyol pathway to galactitol, and the accumulation of galactitol in the lens results in osmotic stress and formation of cataracts. A milder form of galactosemia is caused by galactokinase deficiency. |
|
| Fructose is a component of the disaccharide sucrose, table sugar; it is also found in the diet in the form of common sweetener, high-fructose corn syrup. Fructose is metabolized by two pathways in cells (Fig. 25.7). It may be phosphorylated by hexokinase, an enzyme that is present in all cells; however, hexokinase has a strong preference for glucose, and glucose, which is present at about 5 mmol/L (100 mg/dL) concentration in blood, is a strong competitive inhibitor of the phosphorylation of fructose. The major pathway of
fructose metabolism in liver involves fructokinase, and this pathway is especially important after a meal. Thus, in liver, fructose is phosphorylated to fructose-1-phosphate (Fru-1-P) by fructokinase, and the liver aldolase, called aldolase B, can cleave Fru-1-P, as well as fructose-1,6-bisphosphate (Fru-1,6-BP). In contrast, muscle aldolase, called aldolase A, is specific for Fru-1,6-BP. The products of aldolase B are dihydroxyacetone phosphate and glyceraldehyde (not glyceraldehyde phosphate). The glyceraldehyde must then be phosphorylated by triose kinase in order to be metabolized in the glycolytic pathway.
|
| page 364 | | | page 365 |
| Lactose synthase α-lactalbumin |
| Lactose (galactosyl-β1,4-glucose) is synthesized from UDP-Gal and glucose in mammary glands during lactation. Lactose synthase is formed by the binding of α-lactalbumin to the galactosyl transferase that normally participates in biosynthesis of N-linked glycoproteins. α-Lactalbumin, which is expressed only in the mammary glands during lactation, converts galactosyl transferase to lactose synthase by lowering the enzyme's Km for glucose by about three orders of magnitude, from 1 mol/L to 1 mmol/L, leading to preferential synthesis of lactose. α-Lactalbumin is the only known example of a 'specifier' protein that alters the substrate specificity of an enzyme. |
|
| It should be noted that in the liver, fructose enters glycolysis at the level of triose phosphate intermediates, i.e. after the control points for the regulatory enzymes, hexokinase and phosphofructokinase-1 (PFK-1). By circumventing these two rate-limiting and regulatory enzymes, fructose provides a rapid source of energy for both aerobic and anaerobic cells. This is part of the rationale behind the development
of high-fructose drinks, such as 'Gatorade'. The significance of the fructokinase, as opposed to the hexokinase, pathway of fructose metabolism is indicated by the pathology associated with genetic defects in fructokinase or aldolase B. Fructokinase deficiency leads to a relatively asymptomatic condition, fructosuria. However, a defect in aldolase B causes accumulation of Fru-1-P in the liver, leading to problems similar to those seen in galactosemia. Fortunately, both galactosemia and hereditary fructose intolerance can be managed by removing galactose or fructose, respectively, from the diet.
|
|