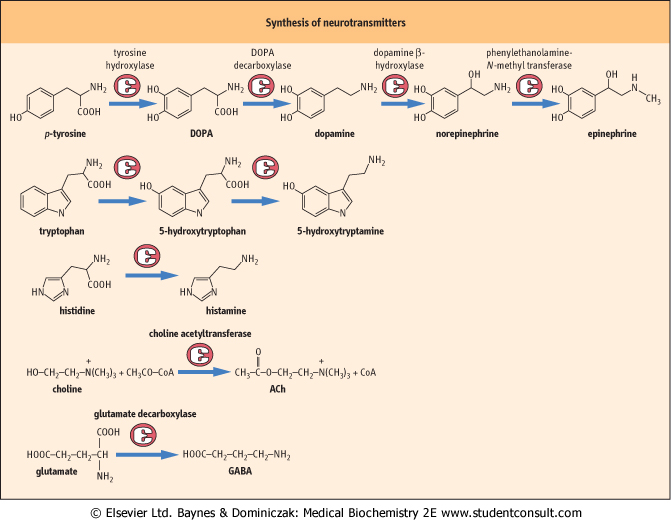
Norepinephrine, epinephrine , and dopamine, known as catecholamines, are all derived from the amino acid tyrosine (see Fig. 40.7). In common with other compounds containing amino groups, such as serotonin, they are also known as biogenic amines. Nerves that release catecholamines have varicosities along the axon, instead of a single area of release at the end. Transmitter is released from the varicosities, and diffuses through the extracellular space until it meets a receptor. This allows it to affect a wide area of tissue, and these compounds are believed to have a general modulatory effect on overall brain functions such as mood and arousal. , and dopamine, known as catecholamines, are all derived from the amino acid tyrosine (see Fig. 40.7). In common with other compounds containing amino groups, such as serotonin, they are also known as biogenic amines. Nerves that release catecholamines have varicosities along the axon, instead of a single area of release at the end. Transmitter is released from the varicosities, and diffuses through the extracellular space until it meets a receptor. This allows it to affect a wide area of tissue, and these compounds are believed to have a general modulatory effect on overall brain functions such as mood and arousal.
|
| page 574 |  | | page 575 |
| Figure 40.7 Synthesis of neurotransmitters. Pathways of synthesis of neurotransmitters are simple. |
| DISORDERS OF NEUROTRANSMISSION |
| Depression as a disease of amine neurotransmitters |
| Monoamine oxidase (MAO) inhibitors prevent the catabolism of catecholamines and serotonin. They therefore increase the concentrations of these compounds at the synapse and increase the action of the transmitters. Compounds with this property are antidepressants. Reserpine, an antihypertensive drug that depletes catecholamines, caused depression and is no longer in use. These dual findings gave rise to the 'amine theory of depression': this states that depression is caused by a relative deficiency of amine neurotransmitters at central synapses, and predicts that drugs which increase amine concentrations should improve symptoms of the condition. |
| In support of this theory, tricyclic antidepressants inhibit transport of both norepinephrine and serotonin into neurons, thereby increasing the concentration of amines in the synaptic cleft. Specific serotonin reuptake inhibitors (SSRIs), such as fluoxetine (Prozac), are also highly effective antidepressants. However, as the symptoms of depression do not resolve for several days after treatment is started, it is likely that long-term adaptations of concentrations of transmitters and their receptors are at least as important as acute changes in amine concentrations in the synaptic cleft. |
| This role of monoamines in depression is undoubtedly an oversimplification. Thus, cocaine is also an effective reuptake inhibitor, but is not an antidepressant, and amphetamines both block reuptake and cause release of catecholamines from nerve terminals, but cause mania rather than relief of depression. |
| page 575 | | | page 576 |
| AN UNUSUAL REACTION TO CHEESE |
| A 50-year-old man had been suffering from depression for some years. His condition was treated with tranylcypromine, an inhibitor of monoamine oxidase types A and B. He developed a severe, throbbing headache and his blood pressure was found to be 200/110 mmHg. The only unusual occurrence had been that he had attended a cocktail party the previous evening at which he ate cheese snacks and drank several glasses of red wine. |
| Comment. The patient was experiencing a hypertensive crisis caused by an interaction between the food he had eaten and the drug he was treated with - a MAO inhibitor. This drug inhibits the main enzyme that catabolizes catecholamines. Several foods, including cheese, pickled herring, and red wine, contain an amine called tyramine, which is similar in structure to natural amine transmitters and is also broken down by MAO. If this enzyme is not functional, the concentrations of tyramine increase and it starts to act as a neurotransmitter. This can cause a hypertensive crisis, as it did in this patient. |
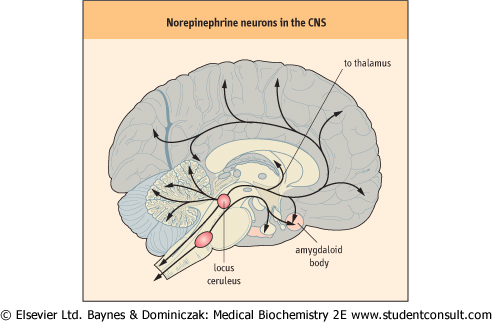
| Figure 40.8 Norepinephrine neurons in the CNS. Norepinephrine-containing neurons arise in the locus ceruleus in the brain stem and are distributed throughout the cortex. |
| Norepinephrine and epinephrine
|
| A NEUROTRANSMITTER CAUSE OF HYPERTENSION |
| A 56-year-old woman presented with severe hypertension. She suffered from attacks of sweating, headaches, and palpitations. Her high blood pressure had not responded to treatment with an angiotensin converting enzyme inhibitor and a diuretic. A sample of urine was taken for measurement of catecholamines and metabolites. The rate of excretion of norepinephrine was 1500 nmol/24 h (253 mg/24 h); (reference range <900 nmol/24 h [<152 mg/24 h]), that of epinephrine 620 nmol/24 h (113 mg/24 h); (reference range <230 nmol/24 h [<42 mg/24 h]) and that of vanillylmandelic acid 60 mmol/24 h (11.9 mg/24 h); (reference range <35.5 mmol/24 h [<7.0 mg/24 h]). |
| Comment. The patient had a pheochromocytoma which is a tumor of the adrenal medulla that secretes catecholamines. Both norepinephrine and epinephrine may be secreted: norepinephrine causes hypertension by activating α-1-adrenoceptors on vascular smooth muscle, and epinephrine increases heart rate by activating β-1-adrenoceptors on the heart muscle. Hypertension may be paroxysmal and severe, leading to stroke or heart failure. |
| Diagnosis is made by measuring catecholamines in plasma or urine, or their metabolites, such as metanephrines and vanillylmandelic acid, in urine. The tumor is usually localized by radiological techniques such as magnetic resonance (MR) or computed tomography (CT) scanning. |
| Although this is a rare cause of hypertension, comprising only about 1% of cases, it is very important to remember it, as the condition is dangerous and often amenable to surgical cure. |
| Norepinephrine (also known as noradrenaline) is a major transmitter in the sympathetic nervous system. Sympathetic nerves arise in the spinal cord and run to ganglia situated close to the cord, from which postganglionic nerves run to the
target tissues. Norepinephrine is the transmitter for these postganglionic nerves, whereas the transmitter at the intermediate ganglia is ACh. Stimulation of these nerves is responsible for various features of the 'fight or flight' response, such as stimulation of the heart rate, sweating, vasoconstriction in the skin, and bronchodilation.
|
| There are also norepinephrine-containing neurons in the CNS, largely in the brain stem (Fig. 40.8). Their axons extend in a wide network throughout the cortex, and alter the overall state of alertness or attention. The stimulatory effects of amphetamines are caused by their close chemical similarity to catecholamines.
|
| page 576 | | | page 577 |
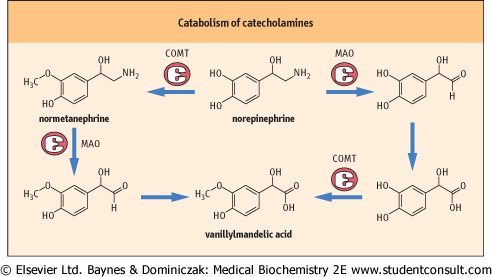
| Figure 40.9 Catabolism of catecholamines. Catecholamines are degraded by oxidation of the amino group by the enzyme monoamine oxidase (MAO), and by methylation by catecholamine-O-methyl transferase (COMT). The pathway shown is for norepinephrine, but the pathways for epinephrine, dopamine, and 5-HT are analogous. |
| Epinephrine (also known as adrenaline) is produced by the adrenal medulla under the influence of ACh-containing nerves analogous to the sympathetic preganglionic nerves. It is more active than norepinephrine on the heart and lungs, causes redirection of blood from the skin to skeletal muscle, and has important stimulatory effects on glycogen metabolism
in the liver. In response to epinephrine, a sudden extra supply of glucose is delivered to muscle, the heart and lungs work harder to pump oxygen round the circulation, and the body is then prepared to run or to defend itself (see Chapter 20). Epinephrine is not essential for life, however, as it is possible to remove the adrenal medulla without serious consequences.
|
| The receptors for norepinephrine and epinephrine are called adrenoceptors. They are divided into α- and β-receptor classes and subclasses on the basis of their pharmacology. Epinephrine acts on all classes of the receptors, but norepinephrine is more specific for α-receptors. β-Blockers, such as atenolol, are used to treat hypertension and chest pain (angina) in ischemic heart disease because they antagonize the stimulatory effects of catecholamines on the heart. Nonspecific α-blockers have limited use, although the more specific α1-blockers such as prazosin, and α2-blockers such as clonidine, can be used to treat hypertension. Certain subclasses of β-receptors are found in particular tissues; for instance, the β2-receptor is present in lung, and β2-receptor agonists such as salbutamol are therefore used to produce bronchial dilatation in asthma without stimulating the β1-receptor in the heart.
|
| Norepinephrine is taken up into cells by a high-affinity transporter and catabolized by the enzyme monoamine oxidase (MAO). Further oxidation and methylation by catecholamine-O-methyl transferase (COMT) convert the products to metanephrines and vanillylmandelic acid (4-hydroxy-3-methoxymandelic acid) (Fig. 40.9), which can be measured in the urine as indices of the function of the adrenal medulla. They are particularly increased in patients who have the tumor of the adrenal medulla known as pheochromocytoma. This tumor causes hypertension because of the vasoconstrictor action of the catecholamines it produces.
|
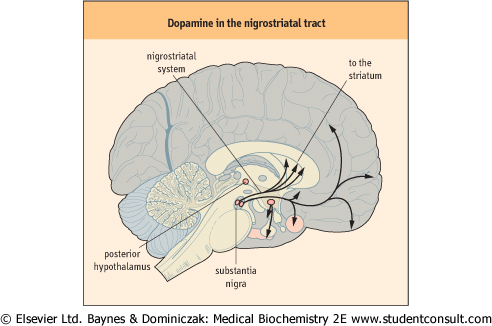
| Figure 40.10 Dopamine in the nigrostriatal tract. Nerves containing dopamine run in well-defined tracts. One of the most important tracts, the nigrostriatal, connects the substantia nigra in the mid brain with the basal ganglia below the cortex. Damage to this causes Parkinson's disease, with loss of fine control of movement. |
| page 577 | | | page 578 |
| Dopamine is both an intermediate in the synthesis of norepinephrine and a neurotransmitter. It is a major transmitter in nerves that interconnect the nuclei of the basal ganglia in the brain and control voluntary movement (Fig. 40.10). Damage to these nerves causes Parkinson's disease, which is characterized by tremor and difficulties in initiating and controlling movement. Dopamine is also found in pathways affecting the
limbic systems of the brain, which are involved in emotional responses and memory. Defects in dopaminergic systems are implicated in schizophrenia, because many antipsychotic drugs used to treat this disease have been found to bind to dopamine receptors.
|
| In the periphery, dopamine causes vasodilatation, and it is therefore used clinically to stimulate renal blood flow, and is important in the treatment of renal failure (Chapter 22). The catabolism of dopamine is comparable to norepinephrine. However, the major metabolite formed is homovanillic acid (HVA).
|
| Serotonin (5-hydroxytryptamine)
|
| Serotonin, also called 5-hydroxytryptamine (5-HT), is derived from tryptophan (see Fig. 40.7). In addition, serotonin biosynthesis has a number of biochemical similarities to dopamine synthesis. Thus, tryptophan hydroxylase like tyrosine hydroxylase displays a cofactor requirement for tetrahydrobiopterin (BH4) (see below). Furthermore, 5-hydroxytryptophan is converted to serotonin by dopa decarboxylase (also known as aromatic amino acid decarboxylase).
|
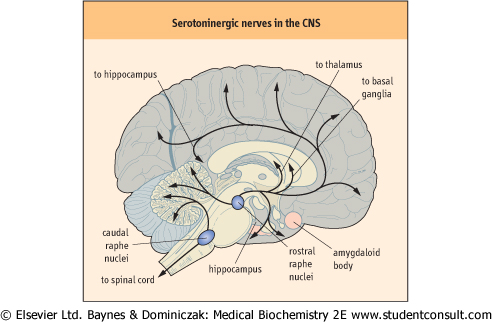
| Figure 40.11 Serotoninergic nerves in the CNS. Serotonin-containing nerves arise in the raphe nuclei, part of the reticular formation in the upper brain stem. In common with those containing norepinephrine, they are distributed widely. |
| MULTIPLE RECEPTORS FOR CATECHOLAMINES AND SEROTONIN |
| Dopamine and serotonin receptors |
| Multiple receptors have been isolated for dopamine and serotonin. Not all those that have been cloned have yet been shown to be functional, but the possible relevance in terms of drug development is obvious. In some cases, specific actions on particular receptors can be exploited therapeutically. |
| There are five known dopamine receptors, falling into two main groups - D1-like (D1 and D5) and D2-like (D2, D3, and D4) - that differ in their signaling pathways. D1 receptors increase the production of cAMP, whereas D2 receptors inhibit it. Antipsychotic drugs such as phenothiazines and haloperidol tend to inhibit D2-like receptors, suggesting that excessive dopamine activity may be important in causing the symptoms of schizophrenia. |
| The D2 receptor is a major receptor in the nerves that interconnect the basal ganglia. As it is known that destruction of these nerves causes Parkinson's disease, it is not surprising that antipsychotic drugs that inhibit the D2 receptor tend to have the side effect of causing abnormal movements. Drugs, such as clozapine, that bind preferentially to the D4 receptor appear to be free of such side effects, although that particular drug also binds to several other receptors. |
| More than a dozen serotonin (5-HT) receptors have been isolated using molecular biological techniques. They have been divided into classes and subclasses on the basis of their pharmacologic properties and their structures. Most are metabotropic, although the 5-HT3 receptor is ionotropic and mediates a fast signal in the enteric nervous system. The 5-HT1A receptor is found on many presynaptic neurons, where it acts as an autoreceptor to inhibit the release of 5-HT. |
| In general, increasing the brain concentration of 5-HT appears to increase anxiety, whereas reducing its concentration is helpful in treating the condition. The antidepressant, buspirone, acts as an agonist at 5-HT1A receptors, and presumably causes a decrease in production of 5-HT. In addition to its effects on the D4 dopamine receptor, clozapine binds strongly to the 5-HT2A receptor, and it may be that a combination of a high level of 5-HT2a antagonism and low D2-binding activity is desirable for drugs that can be used to treat schizophrenia with the minimum frequency of side effects. The 5-HT3 blocker, ondansetron, is an anti-emetic, extensively used to prevent vomiting during chemotherapy. Migraine can be treated with sumatriptan, a 5-HT1D agonist. |
| The central role of 5-HT in controlling brain function and the huge number of associated receptors suggest that it may possible to tailor a large number of drugs to treat specific disorders, and that pharmacological manipulation of the function of the nervous system is probably still in its infancy. |
| page 578 | | | page 579 |
| ANALYSIS OF CEREBROSPINAL FLUID FOR THE DETECTION OF DISORDERS OF DOPAMINE AND SEROTONIN METABOLISM |
| Cerebrospinal fluid (CSF) flows around the major structures of the brain and spinal cord (see also Chapter 39). During circulation, molecules reflecting cellular metabolism diffuse into the CSF. Included in this range of metabolites are the dopamine and serotonin degradation products, homovanillic acid (HVA) and 5-hydroxyindoleacetic acid (5-HIAA). Furthermore, tetrahydrobiopterin (BH4) precursors, metabolites and BH4 itself are also released into the CSF. Thus, determination of such molecules in CSF provides a powerful indicator of the integrity of dopamine and serotonin metabolism within the central nervous system. Such analyses have identified a number of inborn errors of metabolism affecting dopamine and/or serotonin availability, e.g. disorders of BH4 metabolism, pyridoxal phosphate metabolism, tyrosine hydroxylase deficiency and aromatic amino acid decarboxylase (dopa decarboxylase) deficiency. Quantification of the above metabolites is usually achieved by high-performance liquid chromatography (HPLC). For the above molecules, there is a concentration gradient in the CSF, known as the rostral-caudal gradient. Thus, CSF fractions taken from closer to the brain have a high concentration of these metabolites. Furthermore, for many of these metabolites, their concentration declines with age. Consequently, in view of these factors, specialist laboratories providing a diagnostic service require that the same fraction of CSF is provided for analysis. In addition, appropriate age-related reference ranges must be available for correct interpretation of the results generated. |
| Serotoninergic neurons are concentrated in the raphe nuclei in the upper brain stem (Fig. 40.11), but project up to the cerebral cortex and down to the spinal cord. They are more active when subjects are awake than when they are asleep, and serotonin may control the degree of responsiveness of motor neurons in the spinal cord. In addition, it is
implicated in so-called vegetative behaviors such as feeding, sexual behavior, and temperature control.
|
| Serotonin has effects on mood. Reuptake inhibitors, which increase its concentration at the synapse, relieve depression. An excess of serotonin may cause panic attacks; these can be controlled by 5-HT1A-receptor agonists, which are believed to act on autoreceptors to reduce the production of serotonin.
|
| Serotonin also has substantial effects on the peripheral nervous system and enteric neurons. It is a powerful vasoconstrictor, and increases motility of the gastrointestinal tract. Some of the serotonin in the gut arises not from neurons, but from enterochromaffin cells, which are similar to the chromaffin cells in the adrenal medulla that produce epinephrine.
|
| The degradation pathway of serotonin is similar to that of catecholamines, resulting in the formation of 5-hydroxyindoleacetic acid (5-HIAA). This is a useful marker of excessive production or deficiency of serotonin.
|
| FLUSHING ATTACKS CAUSED BY A TUMOR |
| A 60-year-old man complained of attacks of flushing, associated with an increased heart rate. He also had troublesome diarrhea and abdominal pain, and had lost weight. The symptoms suggested a diagnosis of carcinoid syndrome caused by excessive secretion of serotonin and other metabolically active compounds from a tumor. To confirm this, a urine sample was taken for measurement of 5-hydroxyindoleacetic acid (5-HIAA), the major metabolite of 5-HT; the concentration was found to be 120 mmol/24 h (23 mg/24 h); (reference range 10-52 mmol/24 h [3-14 mg/24 h]). |
| Comment. The patient had the carcinoid syndrome, which is caused by tumors of enterochromaffin cells usually originating in the ileum which have metastasized to the liver. These cells are related to the catecholamine-producing chromaffin cells in the adrenal medulla and convert tryptophan to serotonin (5-HT). Serotonin itself is believed to cause diarrhea, but other mediators, such as histamine and bradykinin, may be more important in the flushing attacks. The urinary concentration of 5-HIAA provides a useful diagnostic test and can be used to monitor the response of the cancer to treatment. |
|