| Platelet-related bleeding disorders
|
| Congenital defects in platelet adhesion/aggregation can cause lifelong excessive bleeding
|
A simple screening test - measurement of the skin bleeding time (normal range, 2-10 minutes) - is sufficient to detect congenital defects of platelet adhesion/aggregation, in which the time is characteristically prolonged. The most common such defect is von Willebrand disease (see Table 6.1), a group of autosomal dominant disorders that result in low plasma concentrations of vWF multimers. These multimers are composed of subunits (molecular weight 250 kDa) that are released from endothelial cells (and platelet granules) and circulate in plasma at a concentration of 1 mg/dL. Not only does vWF have an important role in platelet hemostatic function but it also transports coagulation factor VIII (antihemophilic factor) in the circulation and delivers it to sites of vascular injury. Hence, plasma concentrations of factor VIII may also be low in von Willebrand disease. Treatment of this disease is to increase the low plasma vWF activity, usually by means of desmopressin (a synthetic analogue of vasopressin (see Chapter 23) which releases vWF from endothelial cells into plasma). Sometimes this is done using human plasma concentrates. (see Chapter 23) which releases vWF from endothelial cells into plasma). Sometimes this is done using human plasma concentrates.
|
| Less common congenital bleeding disorders include GPIb-IX deficiency (Bernard-Soulier syndrome), GPIIb-IIIa deficiency (Glanzmann's thrombasthenia), and fibrinogen deficiency (because fibrinogen bridges GPIIb-IIIa receptors of adjacent platelets).
|
| page 67 |  | | page 68 |
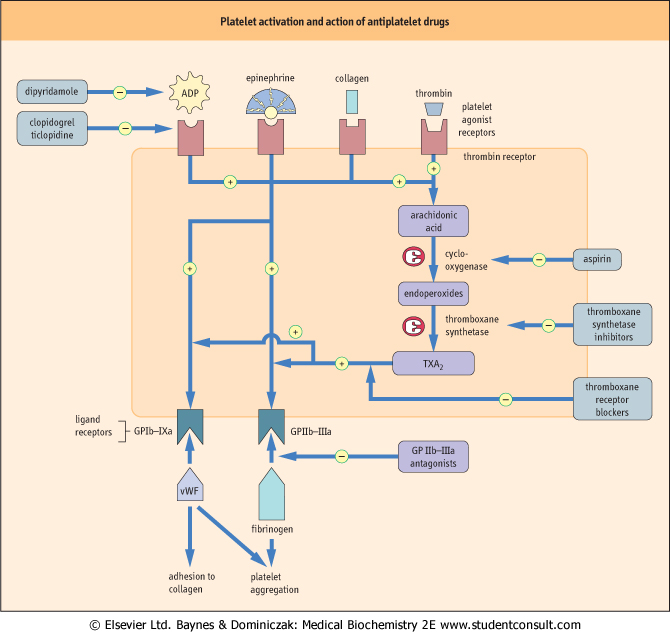
| Figure 6.3 Pathways of platelet activation and mechanisms of action of antiplatelet drugs. Stimulation of platelet agonist receptors results in exposure of platelet ligand receptors, partly through the platelet prostaglandin (cyclo-oxygenase) pathway. Ligand receptors bind vWF and fibrinogen in platelet adhesion/aggregation. |
| Acquired disorders of platelets include a low platelet count (thrombocytopenia), which may be the result either of defective formation of platelets by bone marrow megakaryocytes
(as in marrow neoplasia, or aplasia), or of excessive destruction of platelets (e.g. by antiplatelet antibodies, or in splenomegaly or disseminated intravascular coagulation, DIC).
|
|