| Figure 6.5 Severe bruising that resulted from a minor fall in a 3-year-old child with classic hemophilia. (Courtesy of Dr S Taylor.) |
Thrombin converts circulating fibrinogen to fibrin and activates factor XIII which crosslinks the fibrin forming a clot. It is currently believed that activation of blood coagulation is usually initiated by vascular injury, causing exposure of flowing blood to tissue factor, which results in activation of factors VII and IX. Subsequently, activation of factors X and II (prothrombin) occurs preferentially at sites of
vascular injury, and upon activated platelets, which provide procoagulant activity (platelet factor 3, PF3) as a result of exposure of negatively-charged platelet surface membrane phospholipids, such as phosphatidylserine. This is accompanied by the exposure, on activated platelets, of high-affinity binding sites for several activated coagulation factors (especially factors Va and VIIIa), and provision of platelet phospholipid, which further catalyzes coagulation activation. As a result of these biochemical interactions (see Figs 6.1 and 6.6), thrombin and fibrin formation are efficiently localized at sites of vascular injury. and fibrin formation are efficiently localized at sites of vascular injury.
|
| Thrombin has a central role in hemostasis
|
Not only does thrombin convert circulating fibrinogen to fibrin at sites of vascular injury (producing the secondary, fibrin-rich, hemostatic plug); it also activates factor XIII (transglutaminase), which crosslinks such fibrin, rendering it resistant to dispersion by local blood pressure or by fibrinolysis (see Figs 6.1 and 6.4). Furthermore, thrombin stimulates its own generation in a positive feedback cycle in two ways:
- it catalyzes activation of factor XI; this may explain why congenital deficiencies of factor XII, prekallikrein, or HMWK are not associated with excessive bleeding (Fig. 6.6);
- it catalyzes activation of factors VIII and V.
|
| Thrombin also activates platelets (see Fig. 6.3).
|
| Now that the central role of thrombin in hemostasis and thrombosis has been recognized, there is current interest in the development of direct antithrombins as antithrombotic drugs; these include examples such as hirudin (originally obtained from the medicinal leech, Hirudo medicinalis) and its synthetic derivatives.
|
| page 72 |  | | page 73 |
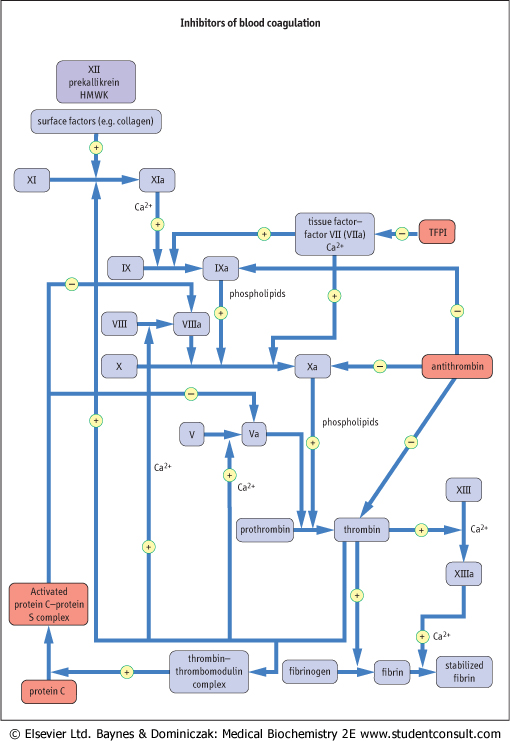
| Figure 6.6 Sites of action of blood coagulation inhibitors: antithrombin, protein C and protein S, and tissue factor pathway inhibitor (TFPI). |
| page 73 | | | page 74 |
|
Table 6-3.
Properties of coagulation inhibitors. |
| Body_ID: None |
| Properties of coagulation inhibitors |
| Body_ID: T006003.50 |
| Inhibitor (synonym) | Molecular weight | Plasma concentration (mg/dL) |
| Body_ID: T006003.100 |
| Anthithrombin (antithrombin III) | 65000 | 18-30 |
| Body_ID: T006003.150 |
| Protein C | 56000 | 0.4 |
| Body_ID: T006003.200 |
| Protein S | 69000 | 2.5 |
| Body_ID: T006003.250 |
| Tissue factor pathway inhibitor, TFPI (lipoprotein-associated coagulation inhibitor, LACI) | 32000 | 0.1 |
| Body_ID: T006003.300 |
| Coagulation inhibitors are essential to prevent excessive thrombin formation and thrombosis
|
| MEASUREMENT OF FIBRIN D-DIMER IN DIAGNOSIS OF SUSPECTED DEEP VEIN THROMBOSIS |
| Fibrin D-dimer (a degradation product of cross-linked fibrin and a marker of fibrin turnover) is normally present in blood at concentrations less than 0.25 g/L. In deep vein thrombosis of the leg (DVT), deposition of a large mass of cross-linked fibrin within the leg veins, followed by partial lysis by the body's fibrinolytic system, increases fibrin turnover and blood D-dimer levels are elevated. Many patients attend accident and emergency departments with a swollen and/or painful leg, which may be due to DVT. Rapid immunoassays for blood D-dimer can be performed in the emergency department, and are now widely used as a adjunct to clinical diagnosis. About one-third of patients with clinically-suspected DVT have normal D-dimer levels, which usually excludes the diagnosis and allows early discharge of such patients without the need for further investigation or treatment. In patients with raised D-dimer levels, heparin treatment is started and imaging of the leg performed (usually by ultrasound) to confirm the presence and extent of DVT. |
|
Three systems of coagulation inhibitors have been identified (see Figs 6.6 and Table 6.3):
- antithrombin: this is a protein synthesized in the liver. Its activity is catalyzed by the antithrombotic drug, heparin, and by heparin-like endogenous glycosaminoglycans (GAGs) that are present on the surface of vascular endothelial cells. It inactivates not only thrombin, but also factors IXa and Xa (see Fig. 6.6). Congenital antithrombin deficiency results in increased risk of venous thromboembolism. Heparin injections are given in the treatment of acute venous or arterial thrombosis; they are usually replaced by oral anticoagulants such as warfarin for longer-term anticoagulation.
- protein C and its cofactor, protein S: these are vitamin-K-dependent proteins, synthesized in the liver. When thrombin is generated, it binds to thrombomodulin (molecular weight 74 kDa), which is present on the surface of vascular endothelial cells. The thrombin-thrombomodulin complex activates protein C, which forms a complex with its cofactor, protein S. This complex selectively degrades factors Va and VIIIa by limited proteolysis (Fig. 6.6). Hence, this pathway forms a negative feedback upon thrombin generation. Congenital deficiencies of protein C or protein S result in increased risk of venous thromboembolism; a further cause of increased risk of venous thromboembolism is a mutation in coagulation factor V (factor V Leiden), which confers resistance to its inactivation by activated protein C. This mutation is common, occurring in about 3% of the population in Western countries.
- tissue factor pathway inhibitor (TFPI): this protein is synthesized in endothelium and the liver; it circulates bound to lipoproteins. It inhibits the tissue factor-VIIa complex (Fig. 6.6), which may explain the severe bleeding in hemophilia caused by deficiency in factor VIII or IX (failure to sustain thrombin and fibrin
formation). Conversely, deficiency of TFPI does not appear to increase the risk of thrombosis.
|
|