| Apoproteins (apolipoproteins)
|
| Apoproteins are the protein components of lipoprotein particles
|
| page 227 |  | | page 228 |
| They interact with cellular receptors and thus determine the metabolic fate of lipoproteins. They also serve as activators and inhibitors of enzymes involved in lipoprotein metabolism.
Main apoproteins are listed in Table 17.4. The most important are apoA, apoB, apoC, apoE, and apo(a). Each class of lipoproteins contains a characteristic set of apoproteins. Apoproteins A (AI and AII) are present in HDL. Apoprotein B variant called apoB100 controls the metabolism of LDL, whereas its truncated form, apoB48 (a N-terminal 48% of apoB100), controls the chylomicrons (see Chapter 33, Fig. 33.7). Apoprotein E controls the receptor binding of remnant particles. Apoproteins C act as enzyme activators and inhibitors and they are extensively exchanged between different lipoprotein classes. Lipoprotein (a) [Lp(a)], may have a role in fibrinolysis (see below).
|
|
Table 17-2.
Phenotypic classification of dyslipidemia. |
| Body_ID: None |
| Phenotypic classification of dyslipidemia |
| Body_ID: T017002.50 |
| Dyslipidemia type (Fredrickson) | Increased electrophoretic fraction (lipoproteins) | Increased cholesterol | Increased triglyceride |
| Body_ID: T017002.100 |
| I | chylomicrons | yes | yes |
| Body_ID: T017002.150 |
| IIa | beta (LDL) | yes | no |
| Body_ID: T017002.200 |
| IIb | pre-beta & beta (VLDL & LDL) | yes | yes |
| Body_ID: T017002.250 |
| III | 'broad beta' band (IDL) | yes | yes |
| Body_ID: T017002.300 |
| IV | pre-beta (VLDL) | no | yes |
| Body_ID: T017002.350 |
| V | pre-beta (VLDL) plus chylomicrons | yes | yes |
| Body_ID: T017002.400 |
|
| Body_ID: T017002.450 |
This is a phenotypic classification developed by Fredrickson and adopted by the WHO; it is based on the electrophoretic separation of serum lipoproteins. For genetic classification refer to Table 17.4.
|
|
Table 17-3.
The most important genetic dyslipidemias. |
| Body_ID: None |
| The most important genetic dyslipidemias |
| Body_ID: T017003.50 |
| Dyslipidemia | Frequency/inheritance | Defect | Plasma lipid pattern | Increased cardiovascular risk |
| Body_ID: T017003.100 |
| Familial | 1:500 | LDL receptor deficiency or | hypercholesterolemia or mixed | yes |
| Body_ID: T017003.150 |
| hypercholesterolemia | autosomal | functional impairment | hyperlipidemia (IIa or IIb) | |
| Body_ID: T017003.200 |
| | dominant | | | |
| Body_ID: T017003.250 |
| Familial combined | 1:50 | overproduction | hypercholesterolemia or mixed | yes |
| Body_ID: T017003.300 |
| hyperlipidemia | autosomal | of apoB100 | hyperlipidemia (IIa or IIb) | |
| Body_ID: T017003.350 |
| | dominant | | | |
| Body_ID: T017003.400 |
| Familial | 1:5000 | presence of E2/E2 isoform | mixed hyperlipidemia (III) | yes |
| Body_ID: T017003.450 |
| dysbetalipoproteinemia | autosomal | defective remnant binding | | |
| Body_ID: T017003.500 |
| (type III hyperlipidemia) | recessive | to LDL receptor | | |
| Body_ID: T017003.550 |
|
| Body_ID: T017003.600 |
|
| Body_ID: T017003.650 |
Mixed hyperlipidemia = increased plasma cholesterol and triglycerides
The three clinically most important dyslipidemias are familial hypercholesterolemia, familial combined hyperlipidemia, and familial dysbetalipoproteinemia.
|
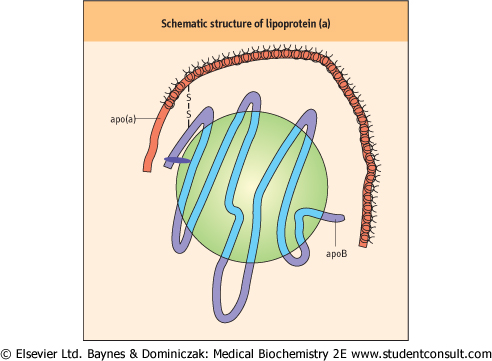
Lipoprotein (a) consists of an LDL particle (containing apoB100) linked through a disulfide bond to another apoprotein, apo(a) (Fig. 17.3). Apo(a) is a glycoprotein with a considerable number of variants of different size (size polymorphism). The molecular mass of these isoforms ranges
between 200 and 800 kDa. Apo(a) possesses a protease domain and a number of repeating sequences of approximately 80-90 amino acids in length, stabilized by disulfide bonds into a triple-loop structure. These structures are called kringles (the name of Danish pastry of similar shape). One of the kringles, kringle IV, is repeated 35 times within the apo(a) sequence. The number of kringle IV repeats determines the size of the lipoprotein (a) isoforms. in length, stabilized by disulfide bonds into a triple-loop structure. These structures are called kringles (the name of Danish pastry of similar shape). One of the kringles, kringle IV, is repeated 35 times within the apo(a) sequence. The number of kringle IV repeats determines the size of the lipoprotein (a) isoforms.
|
| Figure 17.3 Schematic structure of lipoprotein (a). Lipoprotein (a) is essentially an LDL particle, with apo(a) is linked to apoB through a disulfide bridge. Apo(a) is a large molecule containing a number of repeat units (kringles). Kringles have structure similar to plasminogen. |
| page 228 | | | page 229 |
|
Table 17-4.
The function of apoproteins. |
| Body_ID: None |
| Apoproteins |
| Body_ID: T017004.50 |
| Apoprotein | Structural function | Receptor | Effect on enzyme activity |
| Body_ID: T017004.100 |
| AI | HDL | scavenger receptor | LCAT activator |
| Body_ID: T017004.150 |
| | | B1 (SRB1) putative | |
| Body_ID: T017004.200 |
| | | HDL receptor | |
| Body_ID: T017004.250 |
| AII | HDL | HDL receptor? | LCAT cofactor |
| Body_ID: T017004.300 |
| (a) | lp(a) | plasminogen | probably interferes |
| Body_ID: T017004.350 |
| | | receptor? | with fibrinolysis |
| Body_ID: T017004.400 |
| B48 | chylomicrons | LRP | HTGL? |
| Body_ID: T017004.450 |
| B100 | VLDL, IDL, LDL | LDL receptor | - |
| Body_ID: T017004.500 |
| CI, CII | - | - | LPL activation |
| Body_ID: T017004.550 |
| CIII | - | - | LPL inhibition |
| Body_ID: T017004.600 |
| E | remnant particles | LDL receptor | - |
| Body_ID: T017004.650 |
|
| Body_ID: T017004.700 |
Both apoE and apoB bind to LDL (apoB/E) receptor. LCAT, lecithin:cholesterol acyltransferase; LRP, LDL receptor-related protein; HTGL, hepatic triglyceride lipase; LPL, lipoprotein lipase.
|
| PLASMA HOMOCYSTEINE CONCENTRATION IS ANOTHER NON-LIPID MARKER OF CARDIOVASCULAR RISK |
| A rare disease, homocystinuria, where homocysteine accumulates, is associated with premature vascular disease. However, it seems that mild increases in plasma homocysteine are also linked to the increased risk of cardiovascular - and also peripheral vascular disease. |
| Homocysteine metabolism is associated with the metabolism of one-carbon pool. Homocysteine, sulfur-containing amino acid is a product of a metabolism of dietary methionine and is generated as a result of de-methylation of S-adenosyl methionine (Chapter 18, p. 254). Homocysteine can be either metabolized to cystathionine and cysteine, or can be re-methylated to methionine. The re-methylation pathway involves the conversion of N5,10-methylene-tetrahydrofolate (N5,10-MTHF) to N5-MTHF by methylene-tetrahydrofolate reductase (MTHFR). Folate is a co-substrate in this reaction. |
| The common cause of hyperhomocysteinemia is folate deficiency, and also a mutation in the MTHFR gene. Proposed mechanisms of homocysteine toxicity include damage to the endothelium and increased oxidation of LDL. Folic acid is effective in lowering homocysteine. |
| Lipoprotein (a) is assembled in the liver and has a pre-βmobility on electrophoresis. Its density spans the LDL and HDL range (1.04-1.125 g/mL). Its concentration in plasma ranges widely between 0.2 and 120 mg/dL. Apo(a) exhibits a considerable sequence homology with plasminogen. Although it does not possess plasminogen's protease activity, it still may interfere with the action of plasminogen, potentially impairing the process of clot resolution (fibrinolysis) (see Chapter 6).
|
|