Toxicity of glucose is associated with long-term complications of diabetes is associated with long-term complications of diabetes
|
| page 289 |  | | page 290 |
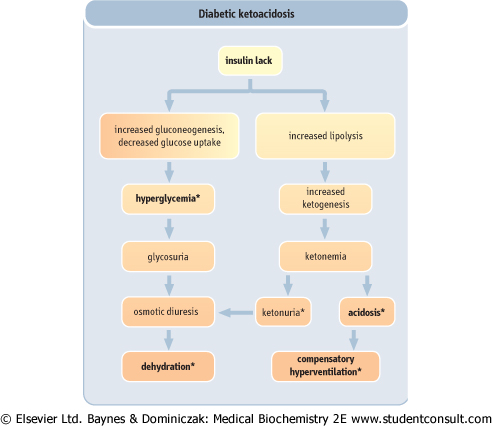
| Figure 20.17 The development of diabetic ketoacidosis. The clinical picture of ketoacidosis is a consequence of hyperglycemia (osmotic diuresis, dehydration) and increased lipolysis (ketonemia and acidosis). *Indicates the most important clinical and laboratory findings. |
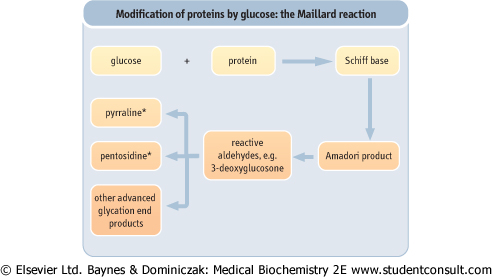
| Figure 20.18 Modification of proteins by glucose: the Maillard reaction. The modification of protein structure and function by sugars leads the formation of the advanced glycation end-products (AGE). (See also Chapter 35.) |
| DIABETIC KETOACIDOSIS AFFECTS BODY POTASSIUM BALANCE |
| Insulin increases potassium uptake by cells. Lack of insulin leads to release of potassium, particularly from skeletal muscle. Since uncontrolled diabetes is accompanied by an osmotic diuresis, the released potassium is excreted through the kidney. Most diabetic patients admitted to hospital with ketoacidosis are potassium-depleted but often have normal or raised levels of plasma potassium. Exogenous insulin given to such patients stimulates the entry of potassium into cells and can lead to very low plasma potassium levels (hypokalemia). Hypokalemia is dangerous, owing to its effects on cardiac muscle. Thus, except for patients with very high potassium levels, potassium supplementation needs to be considered in the treatment of diabetic ketoacidosis. (See Chapters 21 and 22.) |
| PROTEIN MODIFICATION BY GLUCOSE |
| Hyperglycemia promotes the nonenzymatic attachment of glucose to protein molecules (protein glycation). |
| Glucose-protein adducts transform further in a sequence of nonenzymatic reactions (Fig. 20.20), collectively known as the Maillard reaction (so-called after the French chemist, Louis Camille Maillard). Amino acid residues involved include the a-amino terminal amino acid and ε-amino groups of lysine residues. First, a labile Schiff base is formed. This spontaneously transforms to ketoamine through the Amadori rearrangement. Glycated hemoglobin, hemoglobin A1c (HbA1c), is the most widely studied Amadori product. Other proteins, such as albumin and collagen, can also form Amadori products. Glycation changes the electrical charge of proteins and can affect their functions, such as binding to membrane receptors. For instance, glycation of apolipoprotein B slows down the rate of receptor-dependent metabolism of low-density lipoproteins (LDL). (See Chapter 17.) |
| Amadori products transform further to form protein crosslinks known as advanced glycation end products (AGE). AGE crosslink long-lived body proteins such as tissue collagen or a nerve protein, myelin. AGE formation 'stiffens' the extracellular matrix and decreases the elasticity of, for instance, the arterial wall. Their formation also affects the function of endothelial cells, phagocytes (macrophages), and smooth muscle cells in the wall of blood vessels. Through these mechanisms AGE may contribute to the development of the late complications of diabetes and probably other vascular diseases. |
| page 290 | | | page 291 |
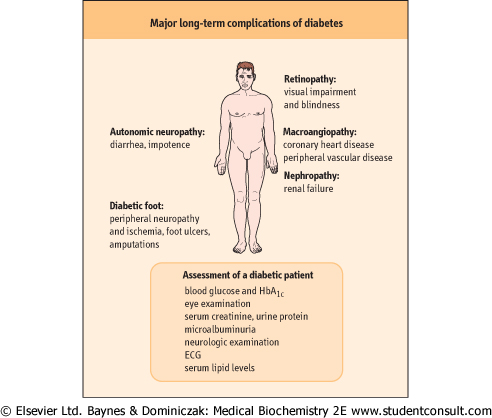
| Figure 20.19 Major long-term complications of diabetes. Late complications of diabetes mellitus include abnormalities of small arteries (microangiopathy: diabetic retinopathy and nephropathy), large arteries (diabetic macroangiopathy: coronary heart disease and peripheral vascular disease), and also in diabetic neuropathy, which results from a combination of vascular and structural tissue changes. |
| Slowly developing changes in small (microangiopathy) and large (macroangiopathy) arteries are part of the diabetic syndrome. In the long term these changes lead to kidney failure (diabetic nephropathy), blindness (caused by diabetic retinopathy), and to the impairment of nerve function (diabetic neuropathy). Diabetic patients also develop lens opacities (cataracts). Owing to macroangiopathy, diabetic individuals are at a two to three times greater risk of myocardial infarction than people who are nondiabetic. Finally, the diabetic peripheral vascular disease is a major cause of foot ulcers and lower limb amputations. Currently, cardiovascular disease is the most prevalent complication, and is the main cause of death among people with diabetes. Diabetes is also
the main cause of blindness in the Western world and one of the main causes of kidney failure. The late complications are illustrated in Figure 20.19.
|
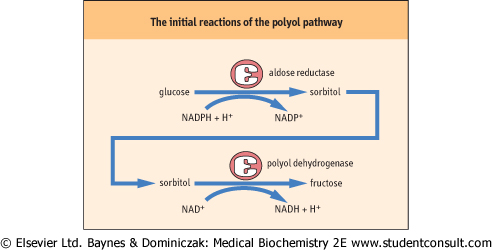
| Figure 20.20 The polyol pathway. The polyol pathway contributes to the development of diabetic neuropathy. This pathway may be inhibited by inhibitors of its rate-limiting enzyme, aldose reductase. |
| POLYOL PATHWAY AND DIABETIC COMPLICATIONS |
| Glucose can be reduced to sorbitol by aldose reductase (Fig. 20.20). Sorbitol is further oxidized by sorbitol dehydrogenase to fructose. Since aldose reductase has a high Km for glucose, the pathway is not very active at normal glucose levels. When there is hyperglycemia, however, glucose levels in insulin-independent tissues (which glucose enters freely), such as the red blood cells, nerve, and lens, increase and consequently there is an increase in the activity of the polyol pathway. Like glucose, sorbitol exerts an osmotic effect. This is thought to play a role in the development of diabetic cataracts. In addition, the high level of sorbitol decreases cellular uptake of another alcohol, myoinositol, which decreases the activity of plasma membrane Na+/K+ ATPase. This in turn affects nerve function and, along with hypoxia and reduced nerve blood flow, contributes to the development of diabetic neuropathy. Drugs inhibiting aldose reductase improve the peripheral nerve function in diabetes. |
|
| Presently considered mechanisms of microvascular complications include the formation of AGE, the oxidative stress, and also the increased substrate flux through polyol pathways (Fig. 20.20). Abnormal activation of the signaling cascades, changing the pattern of synthesis of growth factors and the operation of ion channels emerges as fundamentally important. A recent hypothesis put forward by Michael Brownlee proposes that the production of excess reactive oxygen species by the mitochondrial electron transport chain is the unifying mechanism of diabetic complications (see Further Reading). Hyperglycemia, by affecting the amount of proton donors within the cell, would increase electrochemical potential difference across the inner mitochondrial membrane and would thus lead to an increased production of reactive oxygen species (ROS). ROS would change cellular signaling patterns, leading to the development of insulin
resistance and impaired insulin secretion, and in the long-term, the vascular changes.
|
|