| Insulin resistance signifies inadequate tissue response to the hormone
|
| page 291 |  | | page 292 |
|
Table 20-6.
Sites of insulin resistance. |
| Body_ID: None |
| Sites of insulin resistance |
| Body_ID: T020006.50 |
| Site of resistance | Possible defect | Role in diabetes |
| Body_ID: T020006.100 |
| Prereceptor | insulin receptor antibodies, abnormal molecule | rare |
| Body_ID: T020006.150 |
| Receptor | decreased number or affinity of insulin receptors | not important in diabetes |
| Body_ID: T020006.200 |
| Postreceptor | defects in signal transduction: defective tyrosine phosphylation (?), reduced IRS-1 level, decreased phosphatidylinositol-3' kinase decreased activity of key enzymes such as pyruvate dehydrogenase or glycogen synthase | most probable site of insulin resistance in diabetes |
| Body_ID: T020006.250 |
Glucose transport transport | defective translocation of glucose transporters to cell membrane | important |
| Body_ID: T020006.300 |
|
| Body_ID: T020006.350 |
Cellular insulin resistance may arise at prereceptor or postreceptor level. Insulin resistance is important in obesity, glucose intolerance and type 2 diabetes mellitus. As a component of the metabolic syndrome it is associated with increased risk of cardiovascular disease.
|
| GLYCATED HEMOGLOBIN MEASUREMENT BY AFFINITY CHROMATOGRAPHY |
| Originally HbA1c has been identified by its electrical charge: it migrated faster than the main HbA1 peak on electrophoresis. An ingenious way of measuring glycated hemoglobin is by boronic acid affinity chromatography. The hydroxyl groups in cis-configuration present in the glycated hemoglobin molecule interact with with m-aminophenylboronic acid immobilized on a chromatographic column. Borate produces a complex with the hydroxyl groups favouring the cis configuration. As a result glycated haemoglobin is retained on the column while non-glycated species washes through. Subsequently glycated species is liberated from the columsn and measured spectrophotometrically. Importantly, this method measures all glycated fractions of haemoglobin, not only HbA1c, therefore reference values obtained with this method are different from those obtained by electrophoresis. |
| Insulin resistance, mentioned above in the context of development of type 2 diabetes, is a condition where a given amount of insulin produces a less than expected response. In insulin resistant individuals normal plasma glucose
concentrations is present together with hyperinsulinemia: this is because more insulin is required to produce the 'normal' effect. Insulin resistance is present not only in overt type 2 diabetes mellitus but also in the two conditions which commonly precede diabetes: obesity and impaired glucose tolerance. It also occurs in children of diabetic parents, certifying to its genetic background.
|
| The genetic component to insulin resistance is also confirmed by studies on several strains of knockout mice lacking genes for insulin receptor, GLUT-4, and IRS-1: they all demonstrate insulin resistance. Within a target cell, the resistance may be caused by defects at several levels (Table 20.6). Insulin-receptor binding could be compromised; very rarely a mutation in the insulin-receptor gene causes an extreme insulin resistance. Resistance is also caused by the presence of antireceptor antibodies. However, probably the most important cause of insulin resistance are the defects in insulin receptor signaling: for instance, in persons with type 2 diabetes and those with strong family history of diabetes, abnormal operation of the IRS-phosphoinositol kinase pathway leads to a defective cellular translocation of the GLUT4 transporter, and consequently to the impaired glucose uptake in skeletal muscle and adipose tissue.
|
| Treatment of insulin resistance
|
| Drugs which affect insulin resistance are metformin and recently introduced thiazolidinediones. Thiazolidinediones improve insulin action by binding to the nuclear peroxisome proliferator activator receptor receptor-gamma (PPARγ in the adipose tissue (and, to a lesser extent in muscle), and subsequently increasing transcription of a variety of insulin-sensitive genes responsible for glucose and lipid metabolism. They also activate IRS- phosphoinositol kinase signaling pathway.
|
| There are links between obesity, glucose intolerance, diabetes, and cardiovascular disease
|
| Because diabetes mellitus affects all pathways of fuel metabolism, it should not be just regarded as a discrete, separate disease. First of all, it is closely linked to obesity (obesity is a major risk factor for diabetes). In many obese persons one often observes transition from normal glucose metabolism to impaired glucose tolerance and, subsequently, to diabetes.
|
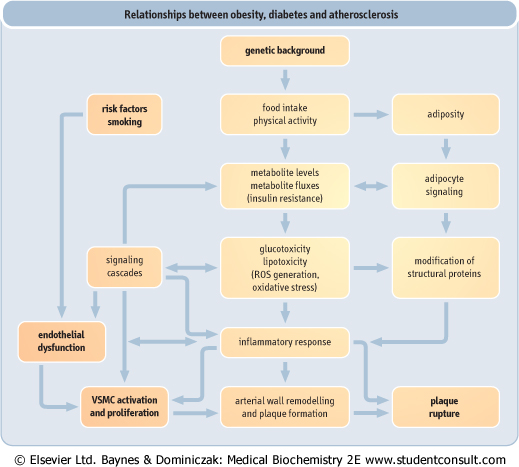
| Also, it is increasingly clear that there are common denominators in diabetes mellitus and cardiovascular disease such as insulin resistance, the low-grade inflammation affecting vasculature (Chapter 17), and the increased tendency to blood coagulation (hypercoagulable state - Chapter 6). In fact, these observations led to the hypotesis proposing 'common soil' for diabetes and cardiovascular disease. The relationships between obesity diabetes and atherosclerosis are illustrated in Figure 20.21.
|
| page 292 | | | page 293 |
| Figure 20.21 Relationships between obesity diabetes and atherosclerosis. Increased food intake and/or decreased physical activity lead to changed metabolite fluxes and adipocyte signaling. Changed metabolism generates glucose- and lipid-derived molecules (glucotoxicity and lipotoxicity) and reactive oxygen species (ROS). ROS further modify body structure proteins and interfere with cell signaling sytems. A low-grade inflammatory response ensues: it has been observed in obesity and diabetes as well as in atherosclerosis. VSMC: vascular smooth muscle cells. (From Dominiczak MH, Obesity, gludose intolerance and diabetes, and their links to cardiovascular disease. Implications for laboratory medicine. Clin Chem Lab Med 2003;41:1266-1278, reprinted with permission.) |
|