| OSMOLALITY AND VOLUME OF ECF AND ICF
|
| The relative volumes of ECF and ICF depend on the amount of osmotically active substances in each of these compartments
|
| All molecules dissolved in the body water contribute to the osmotic pressure, which is proportional to the molal concentration of the solution. One millimole of a substance dissolved in 1 kg H2O at 37°C exerts an osmotic pressure of approximately 19 mmHg. Under physiologic conditions, the average concentration of all osmotically active substances in the ECF is 290 mmol/kg H2O, and this remains in equilibrium with the ICF.
|
| THE COMPOSITION OF BODY FLUIDS DETERMINES ABNORMALITIES RESULTING FROM THEIR LOSS FROM THE BODY |
| Clinical problems caused by the loss of body fluids |
| It is possible to predict problems that may arise from the loss of body fluids. For instance, sweat contains less sodium than extracellular fluid, therefore excessive sweating leads to a predominant loss of water, and 'concentrates' extracellular fluid sodium, leading to increased plasma sodium. In contrast, the sodium content of the intestinal fluid is similar to that of plasma; it contains considerable amounts of potassium. Thus the loss of intestinal fluid (for instance, in severe diarrhea) results in dehydration and hypokalemia, but may not affect plasma sodium concentration (Table 22.1). |
|
Table 22-1.
The electrolyte composition of body fluids. |
| Body_ID: None |
| Electrolyte content of body fluids |
| Body_ID: T022001.50 |
| | Sodium (mmol/L) | Potassium (mmol/L) | Bicarbonate (mmol/L) | Chloride (mmol/L) |
| Body_ID: T022001.100 |
| Plasma | 140 | 4 | 25 | 100 |
| Body_ID: T022001.150 |
| Gastric juice | 50 | 15 | 0-15 | 140 |
| Body_ID: T022001.200 |
| Small intestinal fluid | 140 | 10 | variable | 70 |
| Body_ID: T022001.250 |
| Feces in diarrhea | 50-140 | 30-70 | 20-80 | variable |
| Body_ID: T022001.300 |
| Bile, pleural, and peritoneal fluids | 140 | 5 | 40 | 100 |
| Body_ID: T022001.350 |
| Sweat | 12 | 10 | - | 12 |
| Body_ID: T022001.400 |
|
| Body_ID: T022001.450 |
Loss of fluid that has an electrolyte content similar to that of plasma leads to dehydration with normal plasma electrolyte concentrations. In contrast, dehydration may be accompanied by hypernatremia when the sodium content of the lost fluid is less than that of plasma (e.g. sweat). Overhydration is usually accompanied by hyponatremia. (Adapted with permission from Dominiczak MH, ed. Seminars in clinical biochemistry, 2nd ed. Glasgow: Glasgow University, 1997.)
|
| page 317 |  | | page 318 |
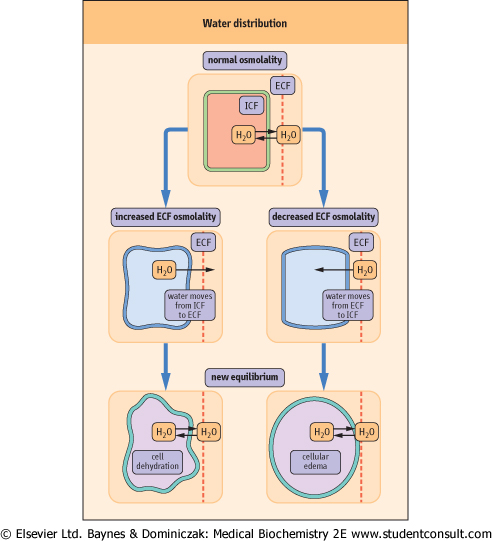
| Figure 22.4 Water redistribution. Osmotic pressure controls the movement of water between different compartments. An increase in ECF osmolality leads to movement of water from the cells into the ECF, and to cellular dehydration. In contrast, when ECF osmolality decreases, water moves from the ECF into the cells. This leads to expansion of the cell volume (edema). Arrows indicate the direction of water movement. |
A change in the concentration of osmotically active ions in either of the compartments creates a gradient of osmotic
pressure and, consequently, induces a movement of water between compartments. Water diffuses from a compartment of low osmolality to one of high osmolality until the osmotic pressures are identical in both of them (i.e. until iso-osmolality is achieved). Thus the relative volumes of ECF and ICF are reflected in the amount of osmotically active substances in these compartments; the sodium ion is the most important in the ECF. Glucose , which is normally present in plasma in a concentration about 5 mmol/L (90 mg/dL), does not contribute much to osmolality, but it may reach very high concentrations in diabetes (in extreme circumstances above
50 mmol/L [900 mg/dL]) and that profoundly affects the osmolality (see Chapter 20) (Fig. 22.4). , which is normally present in plasma in a concentration about 5 mmol/L (90 mg/dL), does not contribute much to osmolality, but it may reach very high concentrations in diabetes (in extreme circumstances above
50 mmol/L [900 mg/dL]) and that profoundly affects the osmolality (see Chapter 20) (Fig. 22.4).
|
| Within the ECF, the distribution of water between intravascular and extravascular compartments depends on the concentration of plasma proteins
|
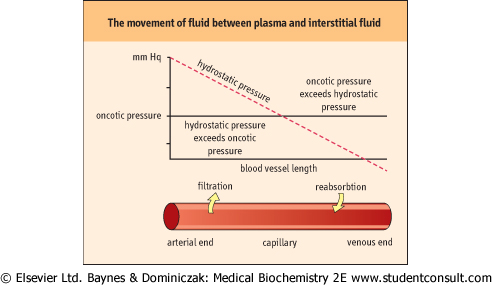
| Figure 22.5 The movement of fluid between plasma and interstitial fluid is determined by the balance between oncotic and hydrostatic pressures. |
| In the plasma, proteins, particularly albumin, exert osmotic pressure (about 3.32 kPa [25 mmHg]), which retains water in the vascular bed; it is known as the oncotic pressure. This is balanced by the hydrostatic pressure, which forces fluid out of the capillaries. In the arterial part of capillaries, the hydrostatic
pressure prevails over the oncotic pressure. As a result, water and low-molecular-weight substances filter out into the extravascular space. In contrast, in the venous part of capillaries, oncotic pressure prevails over hydrostatic pressure, and fluid is drawn into the vascular lumen (Fig. 22.5). A reduction in plasma oncotic pressure, which occurs, for instance, when the plasma concentration of albumin decreases, results in the movement of fluid into the extravascular space; clinically this causes edema.
|
|