| Vasopressin and the renin-angiotensin system in water and electrolyte disorders
|
| Water excess increases plasma volume, renal blood flow, and GFR
|
| DIAGNOSTIC UTILITY OF BNP PROPEPTIDES |
| Instead of measuring the active forms of natriuretic peptides in plasma, it is more convenient to measure the pro-peptides which are present in plasma in equimolar amounts to the active species. Thus proBNP (1-76) reaches higher levels in cardiac failure than BNP 32. Similarly, proANP (1-98) has a longer half-life in plasma than biologically active 1-28 ANP and therefore is present in the circulation in higher concentrations. |
In the condition of water excess the production of rennin, and thus the whole renin-angiotensin-aldosterone axis, is suppressed. The low concentration of aldosterone causes urinary sodium loss. Also, the excess of water 'dilutes' plasma, and plasma osmolality decreases. The decrease in osmolality also suppresses thirst and the secretion of vasopressin
through the action of hypothalamic osmoreceptors. The suppression of vasopressin leads to increased urinary loss of water. The overall response to water excess is therefore a compensatory increase of water and sodium excretion. leads to increased urinary loss of water. The overall response to water excess is therefore a compensatory increase of water and sodium excretion.
|
| On the other hand, water deficit (dehydration) leads to a decrease in plasma volume and thus in renal blood flow and GFR. This stimulates the renin-angiotensin system and the production of aldosterone which inhibits urinary sodium excretion. In addition, because of the loss of water, the plasma osmolality increases and this stimulates vasopressin secretion, with a consequent decrease in the urine volume. Thus the response to water deficit is the retention of sodium and water by the body (Fig. 22.19).
|
| Natriuretic peptides are important markers of heart failure
|
| Another family of peptides, the natriuretic peptides, is involved in the regulation of fluid volume. The two main peptides are the atrial natriuretic peptide (ANP) and the brain natriuretic peptide (BNP). The ANP is synthesized predominantly in the cardiac atria as a 126 amino acid pro-peptide (pro-ANP). It is then cleaved into a smaller 98 amino acid propeptide and the biologically active 28-amino acid ANP. The BNP is synthesized in the cardiac ventricles as 108-amino acid propeptide, and is cleaved into a 76-amino acid propeptide and a biologically active 32-amino acid BNP. BNP 32, and another peptide CNP (22 amino acids long) were also isolated from the porcine brain, thus the name. All natri-uretic peptides possess a ring-type structure due to the presence of a disulfide bond.
|
| page 330 |  | | page 331 |
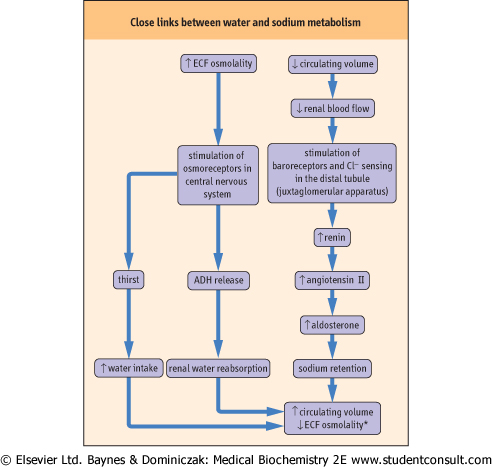
| Figure 22.19 Close links between water and sodium metabolism. The metabolism of water and that of sodium are closely interrelated. An increase in ECF osmolality by only as much as 2% stimulates secretion of vasopressin. Vasopressin increases the renal reabsorption of water through aquaporin-2 water channel. This leads to 'dilution' of the ECF and a decrease in osmolality. This response is reinforced by the stimulation of thirst. Water retention can be induced, not only by an increase in osmolality, but also by a decrease in the volume of circulating plasma, through stimulation of the pressure-sensitive receptors (baroreceptors) in the juxtaglomerular apparatus in the kidney. *Osmolality will decrease if the degree of water retention is relatively greater than sodium retention. |
| Natriuretic peptides promote sodium excretion and induce a decrease blood pressure. ANP and BNP are secreted in response to atrial stretch and ventricular volume overload. They act on the specific receptors which signal through guanyl cyclase and cGTP: the A type receptors are located predominantly in the endothelial cells and the B-type receptors in the brain. There is cross-reactivity between different natriuretic receptors with regard to these peptides. Importantly for clinical diagnosis, the levels of ANP and BNP are increased in heart failure and therefore their measurements are used as biochemical markers of this
condition. These measurements are particularly useful for excluding the presence of mild heart failure in patients who present with nonspecific symptoms such as shortness of breath.
|
| The assessment of water and electrolyte status is an important part of clinical practice
|
| SERUM SODIUM CONCENTRATION IN DISORDERS OF FLUID AND ELECTROLYTE BALANCE |
| Disorders of water and electrolyte metabolism |
| Water and electrolyte disturbances may result from an imbalance between the intake of fluids and electrolytes and their loss through either renal or extrarenal routes, a movement of water and electrolytes between body compartments, or both. A decreased sodium concentration (hyponatremia) usually indicates that the extracellular fluid is being 'diluted', whereas an increasing sodium concentration means that the extracellular fluid is being 'concentrated'. Hyponatremia may result from either excess of water in the system (common), or from the loss of sodium (rare). Conversely, hypernatremia results from either loss of water (common) or excess of sodium (rare). |
The assessment of water and electrolyte balance is an important part of the general examination of a patient. In addition to the physical examination and medical history, the following measurements are required:
- serum electrolyte concentrations: the profile commonly requested a physician includes sodium, potassium, chloride and bicarbonate and also:
- serum creatinine and urea concentration
- urine volume, osmolality and sodium concentration
- serum osmolality
|
| Importantly, patients who stay on a hospital ward and who have or are expected to have abnormal water or electrolyte balance need a fluid chart - that is, a daily record of fluid intake and loss.
|
|