| THE LUNGS AND THE GAS EXCHANGE
|
| The lungs supply oxygen necessary for tissue metabolism and remove the produced CO2; CO2 removal is essential for maintenance of blood pH
|
| Approximately 10000 L of air pass through the lungs of an average person each day. Anatomically, the lungs belong to the lower respiratory tract (as opposed to the upper respiratory tract which comprises nose, pharynx, and larynx) and lie in the thoracic cavity. They are surrounded with the pleural sac, a thin 'bag' of tissue that lines the thoracic cage at one end, and attaches to the external surface of the lungs at the other. When the thoracic cage (chest cavity) expands during inspiration, the negative pressure created in the expanding pleural sac inflates the lung.
|
| page 336 |  | | page 337 |
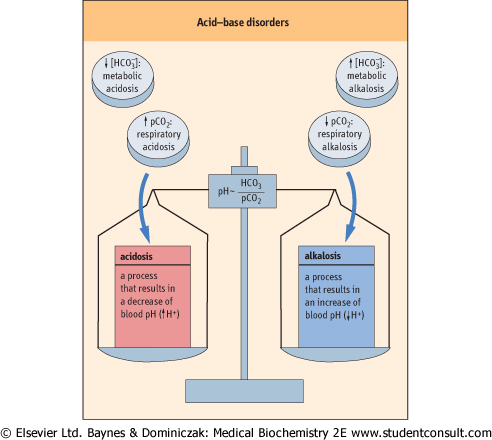
| Figure 23.4 The acid-base disorders. A primary increase in pCO2, or a decrease in plasma bicarbonate concentration, leads to acidosis. A decrease in pCO2, or an increase in plasma bicarbonate, leads to alkalosis. If the primary change is in pCO2, the disorder is called respiratory, and if the primary change is in plasma bicarbonate it is called metabolic. |
|
Table 23-2.
The reference (normal) values for blood gases. |
| Body_ID: None |
| Reference range for blood gas results |
| Body_ID: T023002.50 |
| | Arterial | Venous |
| Body_ID: T023002.100 |
| [H+] | 36-43 mmol/L | 35-45 mmol/L |
| Body_ID: T023002.150 |
| pH | 7.37-7.44 | 7.35-7.45 |
| Body_ID: T023002.200 |
| pCO2 | 4.6-6.0 kPa | 4.8-6.7 kPa |
| Body_ID: T023002.250 |
| pO2 | 10.5-13.5 kPa | 4.0-6.7 kPa |
| Body_ID: T023002.300 |
| bicarbonate | 23-30 mmol/L | |
| Body_ID: T023002.350 |
|
| Body_ID: T023002.400 |
The key clinically used parameters are pH, pCO2 and pO2; the bicarbonate concentration is calculated from pH and pCO2 values; pH below 7.0 or above 7.7 is life threatening. (Adapted with permission from Hutchinson AS. In: Dominiczak MH, ed. Seminars in clinical biochemistry. Glasgow: Glasgow University Press, 1997.)
|
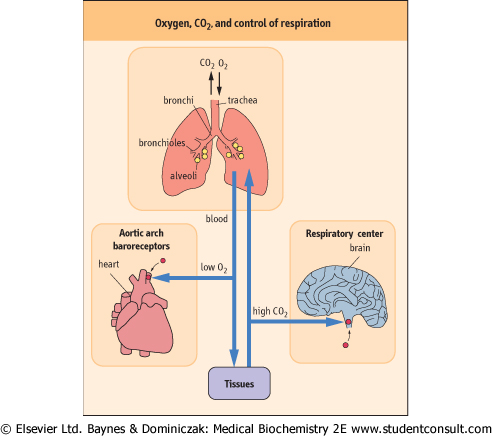
| Figure 23.5 The structure of the lungs and the regulation of the respiratory rate by pCO2 and pO2. Lung ventilation and perfusion are the main factors controlling gas exchange. The pCO2 affects the ventilation rate through the central chemoreceptors in the brainstem. However, when pO2 decreases, the control switches to pO2-sensitive peripheral receptors in the carotid bodies and in the aortic arch. |
| RESPIRATORY ALKALOSIS IS CAUSED BY HYPERVENTILATION |
| A 25-year-old man was admitted to hospital with an asthmatic attack. Peak expiratory flow rate was, measured at 75% of his best. His blood gas values were pO2 9.3 kPa (70 mmHg) and pCO2 4.0 kPa (30 mmHg), with pH 7.50 (hydrogen ion concentration 42 nmol/L). He was treated with nebulized salbutamol, a β2-adrenergic stimulant (see Chapter 39) which is a bronchodilator, and made a good recovery. |
| Comment. This man's blood gases show a mild degree of respiratory alkalosis caused by hyperventilation and 'blowing off' the CO2. Respiratory alkalosis causes reduction in serum levels of ionized calcium leading to neuromuscular irritability. Only in severe asthma does the ventilatory impairment lead to CO2 retention and respiratory acidosis. Reference ranges are given in Table 23.2. |
| page 337 | | | page 338 |
| RESPIRATORY ACIDOSIS OCCURS IN CHRONIC LUNG DISEASES |
| A 56-year-old woman was admitted to a general ward with increasing breathlessness. She had smoked 20 cigarettes a day for the previous 25 years and reported frequent attacks of 'winter bronchitis'. Blood gas measurements revealed a pO2 of 6 kPa (45 mmHg), pCO2 of 8.4 kPa (53 mmHg), and pH 7.35 (hydrogen ion concentration 51 nmol/L); bicarbonate concentration was 35 mmol/L (for reference ranges, refer to Table 23.2). |
| Comment. This patient had an exacerbation of chronic obstructive pulmonary disease and a respiratory acidosis. Her pCO2 was high, and her ventilation was probably dependent on hypoxia, the so-called 'hypoxic drive'. Her bicarbonate was also increased, as a result of metabolic compensation of the respiratory acidosis. It is necessary to be careful when treating such patients with high concentrations of oxygen, because the increased pO2 may remove hypoxic drive and cause respiratory depression. Monitoring of arterial pO2 and pCO2 after oxygen treatment is mandatory. This patient was successfully treated with a 28% concentration of oxygen. |
| The airways are a set of tubes of progressively decreasing diameter. They consist of the trachea, large and small bronchi, and even smaller bronchioles (Fig. 23.5). At the end
of the bronchioles, there are pulmonary alveoli - structures lined with endothelium and covered with a film of surfactant - the main component of which is dipalmitoylphosphatidylcholine (see Chapter 26). Surfactant decreases the surface tension of the alveoli. The epithelium in the bronchi and bronchioles purifies the air by removal of organic and particulate matter. The gas exchange takes place in the alveoli.
|
| The rate of respiration is controlled by the respiratory center in the brainstem. Both pO2 and pCO2 affect respiratory control and thus the ventilation rate: the respiratory center located in the medulla oblongata has chemoreceptors sensitive to pCO2 and to pH. Under normal circumstances, an increase in pCO2 or a decrease in pH (and not the pO2), stimulate ventilation. However, when as the pO2 falls and hypoxia develops, the pO2 begins the control of ventilation through a set of receptors located in the carotid bodies in the aortic arch. When the arterial pO2 decreases to less than 8 kPa (60 mmHg), this 'hypoxic drive' becomes the main mechanism controlling ventilation. Importantly, persons who suffer from long-term hypoxia due to chronic lung disease depend on hypoxic drive to maintain their ventilation rate.
|
| Main factors that determine gas exchange are ventilation and perfusion of the lungs
|
|
Table 23-3.
Partial pressures of oxygen and carbon dioxide in atmospheric air, lung alveoli, and the blood. |
| Body_ID: None |
| Partial pressure gradients determine diffusion of gases through the alveolar-blood barrier |
| Body_ID: T023003.50 |
| | Dry air | Alveoli | Systemic arteries | Tissue |
| Body_ID: T023003.100 |
| pO2 | 21.2 kPa | 13.7 kPa | 12 kPa | 5.3 kPa |
| Body_ID: T023003.150 |
| pCO2 | <0.13 kPa | 5.3 kPa | 5.3 kPa | 6 kPa |
| Body_ID: T023003.200 |
| water vapor | | 6.3 kPa | | |
| Body_ID: T023003.250 |
|
| Body_ID: T023003.300 |
Partial pressure gradients determine diffusion of gases through the alveolar/blood barrier. (1 kPa = 7.5 mmHg)
|
| The blood supply to the alveoli is provided by the pulmonary arteries, blood vessels that carry deoxygenated blood from the periphery through the right ventricle. After oxygenation in
the lungs, the blood flows through pulmonary veins to the left atrium. In the alveolar capillaries of the lungs, the blood accepts oxygen which diffuses through the alveolar wall from the inspired air; at the same time the CO2 diffuses from the blood into the alveoli (see Fig. 23.5) to be removed with the expired air.
|
| The rate of diffusion of gases in and out of the blood is determined by the partial pressure gradient between alveolar air and the arterial blood. Table 23.3 shows the partial pressures of oxygen (pO2) and carbon dioxide (pCO2) in the lungs. Compared with the atmospheric air, the pCO2 in the alveolar air is slightly higher and pO2 slightly lower (this is due to the water vapor pressure). Carbon dioxide is much more soluble than oxygen in water, and equilibrates with blood much more rapidly. Therefore, when problems develop, one first notices a decrease in blood pO2 (hypoxia). An increase in pCO2 (hypercapnia) occurs later and usually indicates a more severe disease.
|
| The other major factor determining gas exchange is the rate at which the blood flows through the lungs (the perfusion rate). Normally, the ratio of ventilation to perfusion (Va/Q) is 0.8: the alveolar ventilation rate is approximately 4 L/min and the perfusion 5 L/min. Table 23.4 shows problems which may develop with gas exchange. Some parts of the lung may be well-perfused, but poorly ventilated. This occurs when some alveoli collapse and are unable to exchange gases. As a result, the pO2 in the outflowing blood is low, because there is no diffusion of oxygen from the alveolar air. The appearance of oxygen-poor blood in the arterial circulation is known as a 'shunt' condition. When ventilation is adequate but perfusion is poor, gas exchange cannot take place: in such cases, part of the lung behaves as if it had no alveoli at all; forming the 'physiologic dead space'.
|
| page 338 | | | page 339 |
In general then, the respiratory problems may be related to poor ventilation, poor perfusion, or the combination of both, and some examples are given below:
- rib-cage deformities impair ventilation by limiting the movement of lungs;
- chest trauma may decrease ventilation as a result of lung collapse; alveoli may be actually destroyed in pulmonary emphysema; inadequate synthesis of surfactant leads to the collapse of alveoli and to the respiratory distress syndrome;
- the bronchial tree may be mechanically obstructed by inhaled objects, or narrowed by a growing tumor: this impairs ventilation or makes it entirely impossible;
- constriction of the bronchi occurs in asthma;
- the ventilatory efficiency may be reduced by impaired elasticity of the lung or the poor function of ventilatory muscles (the diaphragm and intercostal muscles of the chest wall);
- diffusion of gases is more difficult in the presence of fluid in the alveoli (pulmonary edema);
- lung movement is affected by defects in the neural control;
- circulatory problems such as shock and heart failure impair lung perfusion.
|
|
Table 23-4.
Blood partial pressures of oxygen and carbon dioxide depend on lung perfusion and ventilation. |
| Body_ID: None |
| Blood pCO2 and pO2 are affected by the perfusion and ventilation of the lungs |
| Body_ID: T023004.50 |
| | Alveolar pO2 | Alveolar pCO2 | Arterial pO2 | Arterial pCO2 | Comment |
| Body_ID: T023004.100 |
| poor ventilation, adequate perfusion | decreased | increased | decreased | normal | physiologic shunt |
| Body_ID: T023004.150 |
| adequate ventilation, poor perfusion | increased | decreased | decreased* | increased* | physiologic dead space |
| Body_ID: T023004.200 |
*Depending on a degree of shunt.
|
|