| THE CLINICAL DISORDERS OF THE ACID-BASE BALANCE
|
| The lung and the kidney work in a concerted way to minimize changes in plasma pH, and can compensate for each other when problems occur
|
| page 341 |  | | page 342 |
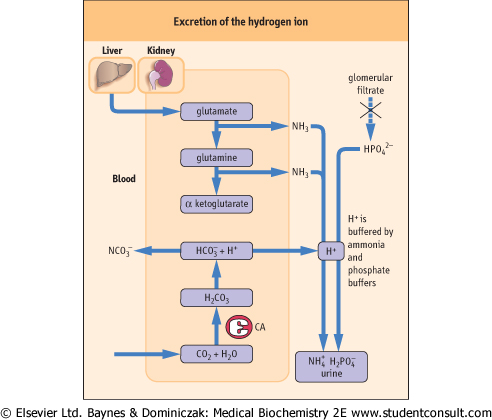
| Figure 23.8 Excretion of the hydrogen ion. Excretion of the hydrogen ion takes place in the distal tubules of the kidney. Hydrogen ion reacts with ammonia forming the ammonium ion which is excreted. Hydrogen ion is also buffered by phosphate. The daily excretion of hydrogen ion is approximately 50 mmol. CA, carbonic anhydrase. |
| THERE IS AN ASSOCIATION BETWEEN ACID-BASE DISORDERS AND PLASMA POTASSIUM CONCENTRATION |
| Plasma potassium concentration is one of the more important clinical laboratory tests. This is because potassium affects the contractility of the heart and either a too high or too low plasma concentration (hyperkalemia and hypokalemia, respectively) can be life threatening. The effects of potassium on heart function can be observed on the electrocardiogram. Hypokalemia leads to an increased excretion of hydrogen ion and, consequently, to metabolic alkalosis. The converse is also true: metabolic alkalosis leads to an increased renal excretion of potassium, and hypokalemia. Plasma potassium concentration needs to be checked whenever a disorder of acid-base balance is suspected (see Fig. 22.13, and Chapter 21). |
|
Table 23-6.
Respiratory and metabolic compensation in the acid base disorders minimizes changes in the blood pH. |
| Body_ID: None |
| Respiratory and metabolic compensation of acid-base disorders |
| Body_ID: T023006.50 |
| Acid/base disorder | Primary change | Compensatory change | Timescale of compensatory change |
| Body_ID: T023006.100 |
| metabolic acidosis | decrease in plasma bicarbonate concentration | decrease in pCO2 (hyperventilation) | minutes/hours |
| Body_ID: T023006.150 |
| metabolic alkalosis | increase in plasma bicarbonate concentration | increase in pCO2 (hypoventilation) | minutes/hours |
| Body_ID: T023006.200 |
| respiratory acidosis | increase in pCO2 | increase in renal bicarbonate reabsorption: increase in plasma bicarbonate concentration | days |
| Body_ID: T023006.250 |
| respiratory alkalosis | decrease in pCO2 | decrease in renal bicarbonate reabsorption: decrease in plasma bicarbonate concentration | days |
| Body_ID: T023006.300 |
|
| Body_ID: T023006.350 |
A change in the respiratory component leads to metabolic compensation, and a change in the metabolic component stimulates respiratory compensation. Metabolic compensation involves a change in renal bicarbonate handling, and respiratory compensation means changes in the ventilation rate. A compensatory increase or decrease in the rate of ventilation (hyper- or hypoventilation) is seen within minutes, however, an adjustment of the rate of bicarbonate reabsorption may take days.
|
| page 342 | | | page 343 |
|
Table 23-7.
The clinical causes of acid-base disorders. |
| Body_ID: None |
| Clinical causes of acid-base disorders |
| Body_ID: T023007.50 |
| Metabolic acidosis | Respiratory acidosis | Metabolic alkalosis | Respiratory alkalosis |
| Body_ID: T023007.100 |
| diabetes mellitus (ketoacidosis) | chronic obstructive airways disease | vomiting (loss of hydrogen ion) | hyperventilation (anxiety, fever) |
| Body_ID: T023007.150 |
lactic acidosis (lactic acid ) ) | severe asthma | nasogastric suction (loss of hydrogen ion) | lung diseases associated with hyperventilation |
| Body_ID: T023007.200 |
| renal failure (inorganic acids) | cardiac arrest | hypokalemia | anemia |
| Body_ID: T023007.250 |
| severe diarrhea (loss of bicarbonate) | depression of respiratory center (drugs, e.g. opiates) | intravenous administration of | salicylate poisoning |
| Body_ID: T023007.300 |
| surgical drainage of intestine (loss of bicarbonate) | weakness of respiratory muscles (e.g. poliomyelitis, multiple sclerosis) | bicarbonate (e.g. after cardiac arrest) | |
| Body_ID: T023007.350 |
| renal loss of bicarbonate (renal tubular acidosis type 2 - rare) | chest deformities | | |
| Body_ID: T023007.400 |
| impairment of renal H+ excretion (renal tubular acidosis type 1 - rare) | airway obstruction | | |
| Body_ID: T023007.450 |
|
| Body_ID: T023007.500 |
Disorders of the acid-base balance are acidosis and alkalosis: each of them can be either respiratory or metabolic. Respiratory acidosis is common and is caused primarily by diseases of the lung that affect gas exchange. Respiratory alkalosis is rarer and is caused by hyperventilation, which decreases pCO2. Metabolic acidosis is common and results from either overproduction or retention of nonvolatile acids in the circulation. Metabolic alkalosis is rarer: its most common causes are vomiting and gastric suction, both causing loss of hydrogen ion from the stomach.
|
| Disturbances of acid-base balance may be caused by primary problems affecting the regulation of pCO2 (the respiratory component) or bicarbonate concentration (the metabolic component). Returning to the Henderson-Hasselbalch
equation, please note that the increased ratio of plasma bicarbonate to pCO2 indicates acidosis, and the decreased ratio, alkalosis.
|
|