| KIDNEYS AND THE HANDLING OF BICARBONATE
|
| The kidneys control plasma bicarbonate concentration and the excretion of hydrogen ion from the body
|
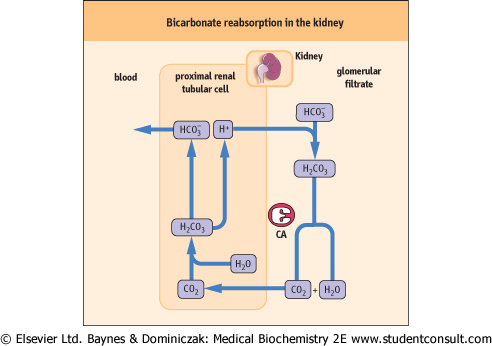
| Figure 23.7 Bicarbonate reabsorption in the kidney. Bicarbonate reabsorption takes place in the proximal tubule. At this stage, there is no net excretion of hydrogen ion. Carbonic anhydrase (CA) is present on the luminal side of the tubular cells (see text for details). |
| The kidneys play an essential role in the control of plasma bicarbonate concentration and in the removal of hydrogen
ion from the body. In common with erythrocytes, the renal (proximal and distal) tubular cells contain carbonic anhydrase which plays a major role in the handling of hydrogen ion.
|
| Bicarbonate reabsorption takes place in the proximal tubule
|
| Normally, urine is almost bicarbonate free; an amount equivalent to that filtered by glomeruli is returned to the plasma by the proximal tubular cells. The surfaces of the renal tubular cells facing the tubule lumen (the luminal surfaces) are impermeable to bicarbonate. However, the filtered bicarbonate ion combines with the hydrogen ion secreted by the proximal tubular cells to form carbonic acid, and this is then converted to freely diffusible CO2 and H2O by carbonic anhydrase located on the luminal membrane. Thus the CO2 diffuses into cells where it is re-converted by carbonic anhydrase into carbonic acid dissociating back into hydrogen and bicarbonate ions. The two ions are now moved in opposite directions: bicarbonate is returned to the plasma, completing the reabsorption process and hydrogen ion is secreted into the lumen of the tubule, to combine with another filtered bicarbonate ion. Therefore in this process hydrogen ion is used exclusively to aid bicarbonate reabsorption, and no net excretion of hydrogen ion takes place (Fig. 23.7).
|
| page 340 |  | | page 341 |
| Bicarbonate generation and hydrogen ion excretion take place in the distal tubule
|
| RESPIRATORY AND METABOLIC DISORDERS OF ACID-BASE BALANCE CAN OCCUR TOGETHER |
| During resuscitation of a 60-year-old man from a cardiorespiratory arrest, the blood gas analysis revealed pH 7.00 (hydrogen ion concentration 100 nmol/L) and pCO2 7.5 kPa (52 mmHg). His bicarbonate concentration was 11 mmol/L. pO2 was 12.1 kPa (91 mmHg) during treatment with 48% oxygen. |
| Comment. This patient had a mixed disorder: a respiratory acidosis caused by lack of ventilation, and metabolic acidosis caused by the hypoxia that had occurred before oxygen treatment was instituted. The acidosis was probably caused by an accumulation of lactic acid: the measured lactate concentration was 7 mmol/L (reference range is 0.7-1.8 mmol/L [6-16 mg/dL]). The terms acidosis and alkalosis do not just describe blood pH changes: they relate to the processes that result in these changes. Therefore, in some instances, two independent processes may occur: for example a patient may be admitted to hospital with diabetic ketoacidosis and coexisting emphysema causing respiratory acidosis. The final result could be a more severe change in pH than would have resulted from a simple disorder (Table 23.5). Any combination of disorders can occur; the skills of an experienced physician are usually required to diagnose this. |
|
Table 23-5.
Mixed metabolic and respiratory acidosis and alkalosis. |
| Body_ID: None |
| Mixed metabolic and respiratory acidosis |
| Body_ID: T023005.50 |
| Disorder | pH | pCO2 | Bicarbonate |
| Body_ID: T023005.100 |
| metabolic acidosis | decrease | decrease (respiratory compensation) | decrease (primary change) |
| Body_ID: T023005.150 |
| respiratory acidosis | decrease | increase (primary change) | increase (metabolic compensation) |
| Body_ID: T023005.200 |
| mixed respiratory and metabolic acidosis | large decrease | increase (respiratory acidosis) | decrease (metabolic acidosis) |
| Body_ID: T023005.250 |
| Mixed metabolic and respiratory alkalosis (rare) |
| Body_ID: T023005.300 |
| Disorder | pH | pCO2 | Bicarbonate |
| Body_ID: T023005.350 |
| metabolic alkalosis | increase | increase (respiratory compensation) | increase (primary change) |
| Body_ID: T023005.400 |
| respiratory alkalosis | increase | decrease (primary change) | decrease (metabolic compensation) |
| Body_ID: T023005.450 |
| mixed respiratory and metabolic alkalosis | large increase | decrease (respiratory alkalosis) | increase (metabolic acidosis) |
| Body_ID: T023005.500 |
|
| Body_ID: T023005.550 |
Mixed acid-base disorders result in a greater change in blood pH than simple disorders; they may pose diagnostic difficulties.
|
| The situation is different in the distal tubules where bicarbonate generation takes place. The mechanism is identical to that of bicarbonate reabsorption but this time there is both a net loss of hydrogen ions from the body and a net gain of bicarbonate. This is how it happens: CO2 diffuses freely into cells. In the distal tubule, carbonic anhydrase converts it into
carbonic acid which dissociates into hydrogen ion and bicarbonate. As in the proximal tubule, bicarbonate is transported to the plasma and hydrogen ion is secreted into the tubule lumen (in exchange for sodium). However, since normally no bicarbonate is present in the lumen of the distal tubule (all has been reabsorbed earlier), the hydrogen ion is buffered instead by the filtered phosphate ions and by ammonia synthesized by the proximal tubule cell. It is subsequently excreted in the urine (Fig. 23.8).
|
| The ammonia derives from the transformation of glutamine into glutamic acid by the enzyme glutaminase. Ammonia diffuses freely through the luminal membrane and the hydrogen ion is trapped inside the tubule as the ammonium ion (NH4+) to which the membrane is impermeable.
|
| Problems with renal handling of bicarbonate and hydrogen ion lead to a group of relatively rare disorders known as renal tubular acidoses (RTA). The distal RTA is due to the impairment of hydrogen ion excretion in the collecting duct, and the proximal RTA to the impaired reabsorption of bicarbonate. Proximal RTA usually occurs together with other defects in proximal transport mechanisms in the so-called Fanconi syndrome.
|
|