| Factors influencIng calcium homeostasis
|
| Calcium-sensing receptor is a cell-surface G-protein receptor
|
| Ionized calcium is maintained within a narrow range through an extracellular calcium-sensing receptor (CaSR) that is a cell surface G-protein coupled receptor present in the chief cells of the parathyroid gland, the thyroidal C-cells and along the kidney tubules. Minute changes in ionized calcium modulate cellular function to maintain normocalcaemia.
|
| PARATHYROID HORMONE MEASUREMENT |
| Intact PTH(1-84) is the most important biologically active form of PTH, and can be measured by specific immunoradiometric assays (IRMAs) without interference from its amino- or carboxy-terminal fragments. These assays utilize a double-antibody technique, with a capture antibody directed against one end of the intact molecule, and the labeled detection antibody directed against the opposite end of the molecule. Only the full-length, 1-84-amino acid molecule can bind to the two antibodies, which means that fragments of PTH produced during its metabolism (see Fig. 24.3) are not measured by these assays. |
| Parathyroid hormone (PTH)
|
| Parathyroid hormone responds to changes in ionized calcium and phosphate
|
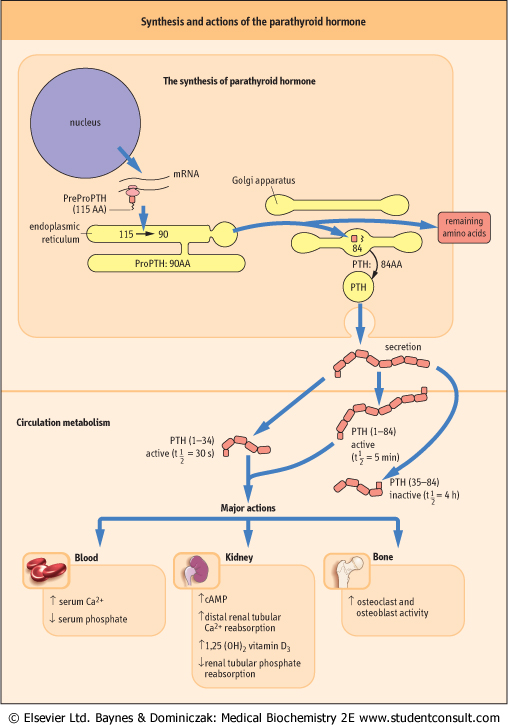
| PTH is an 84-amino-acid, single-chain peptide hormone secreted by the chief cells of the parathyroid glands. A decrease in extracellular ionized calcium or an increase in serum phosphate concentration stimulates its secretion, chronic severe magnesium deficiency can inhibit its release from secretory vesicles, and low concentrations of 1,25(OH)2D3 interfere with its synthesis. PTH(1-84) is mainly metabolized into a biologically active PTH(1-34) aminoterminal fragment and an inactive carboxy-terminal fragment, PTH(35-84) (Fig. 24.4).
|
| PTH regulates serum calcium concentrations by direct actions on bone and kidney, and indirect actions on the intestine by increasing the synthesis of 1,25(OH)2D3 (see Fig. 24.2). Most of the classical cellular actions of PTH are mediated by cAMP, which is generated through G-protein-stimulated adenylyl cyclase.
|
| Vitamin D is synthesized in the skin by UV radiation
|
| page 348 |  | | page 349 |
| Figure 24.4 Synthesis and major actions of parathyroid hormone (PTH). |
| page 349 | | | page 350 |
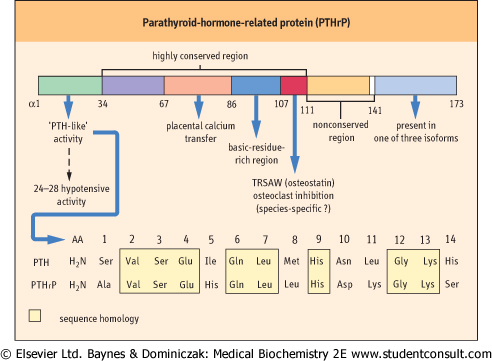
| Figure 24.5 Parathyroid-hormone-related protein (PTHrP) synthesis, structure, and functional relationships. |
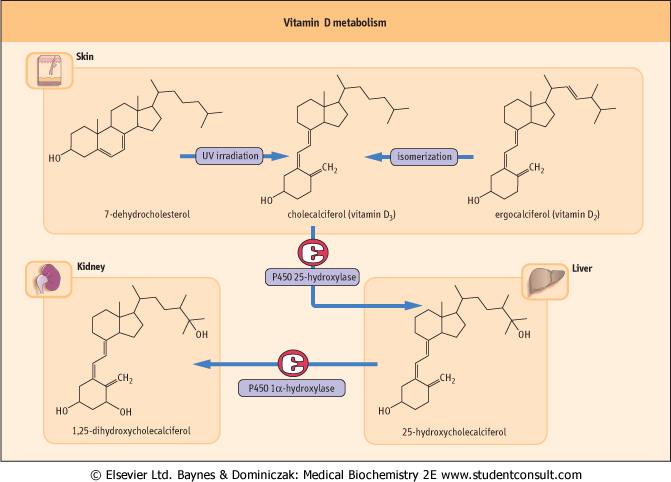
The synthesis and metabolism of vitamin D are illustrated in Figure 24.6. Vitamin D2 (ergocalciferol ) is synthesized in the skin by UV radiation of ergosterol. Vitamin D3 (cholecalciferol) is derived also by UV irradiation from 7-dehydrocholesterol in the skin of animals. Vitamin D3 and its hydroxylated metabolites are transported in the plasma bound to a specific globulin, vitamin D-binding protein (DBP). The affinity of cholecalciferol for DBP is low but that for D3 is high, thus ensuring the movement of D3 from the skin to the circulation. Vitamin D3 is also found in the diet where its absorption is associated with other fats (see Chapter 9), and it is
transported to the liver in chylomicrons. It is released from chylomicrons in the liver by DBP and hydroxylated at the 25-position forming 25-hydroxycholecalciferol ((25(OH)D3; calcidiol). ) is synthesized in the skin by UV radiation of ergosterol. Vitamin D3 (cholecalciferol) is derived also by UV irradiation from 7-dehydrocholesterol in the skin of animals. Vitamin D3 and its hydroxylated metabolites are transported in the plasma bound to a specific globulin, vitamin D-binding protein (DBP). The affinity of cholecalciferol for DBP is low but that for D3 is high, thus ensuring the movement of D3 from the skin to the circulation. Vitamin D3 is also found in the diet where its absorption is associated with other fats (see Chapter 9), and it is
transported to the liver in chylomicrons. It is released from chylomicrons in the liver by DBP and hydroxylated at the 25-position forming 25-hydroxycholecalciferol ((25(OH)D3; calcidiol).
|
| 25-hydroxycholecalciferol (25(OH)D3) is the main liver storage form of vitamin D
|
| The 25-hydroxylation step is carried out by a hepatic microsomal enzyme and is the rate-limiting step in conversion of vitamin D3 to its active metabolite. The hepatic content of 25(OH)D3 regulates the rate of 25-hydroxylation. 25(OH)D3 is the major form of the vitamin found in both the liver and in the circulation, in each case bound to DBP, and its levels in the circulation reflect the hepatic stores of the vitamin. A significant proportion of 25(OH)D3 is subject to an enterohepatic circulation, being excreted in the bile and reabsorbed in the small bowel. Disturbance in the enterohepatic circulation can lead to deficiency of this vitamin.
|
| The active metabolite of vitamin D is 1α,25-dihydroxycholecalciferol (1,25-(OH)2D3)
|
| PARATHYROID-HORMONE-RELATED PROTEIN (PTHrP) |
| PTHrP is synthesized as three isoforms containing 139, 141, and 173 amino acids, as a result of alternative differential splicing of RNA. There is amino-terminal sequence homology with PTH: eight of the first 13 amino acids are identical in PTHrP and PTH, three are identical within residues 14-34, and a further three are identical within residues 35-84. Activation of the classical PTH receptor is by the amino-terminal portion of both PTH and PTHrP, and there is a common α-helical secondary structure in the binding domain of both peptides. As a result of this structural similarity, PTHrP possesses many of the biological actions of PTH. |
| There is, to date, little evidence to suggest that PTHrP has a role in normal adult calcium homeostasis, but evidence from animal models indicates that it is important in regulating fetal skeletal development and calcium homeostasis. Deletion of the PTHrP gene results in either severe skeletal abnormalities (heterozygote) or a lethal mutation (homozygote). PTHrP has an important role in the etiology of hypercalcemia associated with malignancy (HCM) (see below). PTHrP is subject to post-translational processing, producing fragments with biological activities that have yet to be characterized. The structural and functional relationships of PTHrP as they are currently understood are summarized in Figure 24.5. |
| The main site for further hydroxylation at the 1-position are the renal tubules, although bone and the placenta can also carry out this reaction. The 25(OH)D3 1α-hydroxylase is a mitochondrial enzyme. 1,25(OH)2D3; calcitriol is the most potent of the vitamin D metabolites and the only naturally occurring form of vitamin D that is active at physiologic concentrations. The 1α-hydroxylase activity is stimulated by PTH, low serum concentrations of phosphate or calcium, vitamin D deficiency, calcitonin, growth hormone, prolactin,
and estrogen. Conversely, the activity of 1α-hydroxylase is feedback-inhibited by 1,25(OH)2D3, hypercalcemia, high phosphate and hypoparathyroidism.
|
| page 350 | | | page 351 |
| Figure 24.6 Vitamin D metabolism and its action. Vitamin D is mainly synthesized in response to the action of sunlight on the skin; a smaller component comes from the diet. Normal liver and kidney function are essential to the formation of the active form 1,25(OH)2D3. Plasma calcium concentration controls the level of 125 (OH2)D3 through the parathyroid hormone. PTH: parathyroid hormone. DBP: vitamin D-binding protein. |
| The renal tubules, cartilage, intestine, and placenta also contain a 24-hydroxylase, producing the inactive
24,25-dihydroxycholecalciferol (24,25[OH]2D3; 24(R)-hydroxycalcidiol). The level of the 24,25[OH]2D3 in the circulation is reciprocally related to the level of the 1,25(OH)2D3.
|
| 1,25(OH)2D3 is transported in plasma, also bound to DBP. Since it affects Ca2+ transport and metabolism at a distance, vitamin D may be described as a hormone. In the intestinal epithelial cells it binds to a cytoplasmic receptor like other steroid hormones (see Chapter 16) and this ligand-protein complex is transported to the nucleus where 1,25(OH)2D3 induces gene expression affecting calcium metabolism.
|
| 1,25(OH)2D3 increases serum concentrations of calcium and phosphate
|
| 1,25(OH)2D3 increases the absorption of calcium and phosphate from the gut via active transport by calcium-binding proteins. Together with PTH, it stimulates bone resorption by osteoclasts. These effects increase serum calcium and phosphate concentrations. Low 1,25(OH)2D3 causes abnormal mineralization of newly formed osteoid.This is a result of low calcium and phosphate availability and reduced osteoblast function, which result in rickets (in infants and children) or osteomalacia (in adults).
|
| Calcitonin inhibits osteoclastic bone resorption
|
| page 351 | | | page 352 |
| Calcitonin is a 32-amino-acid peptide synthesized and secreted primarily by the parafollicular cells of the thyroid gland (C-cells). Its secretion is regulated acutely by serum calcium through the CaSR: an increase in serum calcium results in a proportional increase in calcitonin, and a decrease elicits a corresponding reduction in calcitonin. Chronic stimulation results in exhaustion of the secretory reserve of the C-cells. The precise biological role of calcitonin is not known, but the main effect is inhibition of osteoclastic bone resorption. There is significant species homology for
calcitonin, with a 1-7 amino-terminal disulfide bridge, a glycine residue at position 28, and a carboxy-terminal proline amide residue. Basic amino acid substitutions enhance potency; because of this, salmon and eel calcitonins have increased biological activity in mammalian systems, compared with that of endogenous calcitonin.
|
| Other hormones also affect calcium homeostasis
|
| Several hormones whose primary action is not related to calcium regulation directly or indirectly affect calcium homeostasis and skeletal metabolism.
|
| Thyroid hormone stimulates osteoclast-mediated resorption of bone. Adrenal and gonadal steroids, particularly estrogen in women and testosterone in men, have important regulatory effects, increasing osteoblast and decreasing osteoclast function. They also decrease renal calcium and phosphate excretion and intestinal calcium excretion. Growth hormone has anabolic effects on bone, promoting growth of the skeleton. These effects of growth hormone on bone are believed to be mediated by insulin-like growth factors (IGF-I and IGF-II) acting on cells of the osteoblast lineage. Growth hormone increases the urinary excretion of calcium and hydroxyproline, whilst decreasing the urinary excretion of phosphate.
|
| Calcium is absorbed in the small intestine and is excreted in urine and feces
|
Calcium is absorbed predominantly in the proximal small intestine; this is regulated through the quantity of calcium ingested in the diet, and two cellular calcium transport processes:
- active saturable transcellular absorption which is stimulated by 1,25(OH)2D3;
- nonsaturable paracellular absorption which is controlled by the concentration of calcium in the intestinal lumen relative to the serum concentration.
|
| In a normal adult taking a Western diet, calcium balance is maintained: the amount of calcium intake and its deposition in bone are exactly matched by the excretion in urine and feces. During growth, a child will be in positive calcium balance, whereas in the elderly and in several diseases, individuals may be in negative calcium balance. Reduced or increased calcium absorption reflects alterations in dietary calcium intake, intestinal calcium solubility, and vitamin D metabolism.
|
| Generally, as serum calcium increases, calcium excretion increases. When hypercalcemia is caused by hyperparathyroidism (HPT), PTH will act on the renal tubule, promoting reabsorption of filtered calcium and thus diminishing the effects of the increased filtration of calcium and inhibition of renal tubular reabsorption that are caused by increased serum calcium. Decreasing serum calcium is associated with a reduction in urinary excretion of calcium, mainly as a result of decreased amounts of filtered calcium. In hypoparathyroid patients, who lack PTH secretion, renal tubular reabsorption of calcium is reduced.
|
|