| Excess intake of alcohol remains the most common cause of liver disease in the Western world
|
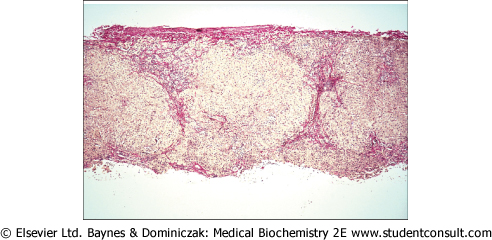
| Excess intake of alcohol remains the most common cause of liver disease in the Western world and may cause alcoholic hepatitis, steatosis due to deposition of fat or finally fibrosis (known as cirrhosis) which in turn leads to liver failure. The microscopic features of alcoholic cirrhosis are shown in Figure 28.8.
|
| page 406 |  | | page 407 |
| Figure 28.8 A histological slide of a cirrhotic liver. (Courtesy Dr J Newman, Birmingham Heartlands and Solihull NHS Trust, UK). |
| Alcohol is oxidized in the liver, mainly by alcohol dehydrogenase, to form acetaldehyde, which is in turn oxidized by aldehyde dehydrogenase (ALDH) to acetate. Nicotinamide adenine dinucleotide (NAD+) is the cofactor for both these
oxidations, being reduced to NADH. A P450 cytochrome, CYP2E1, also contributes to ethanol oxidation, but is quantitatively less important than the alcohol dehydrogenase/ALDH pathway. Liver damage in patients who are abusers of alcohol may arise from the toxicity of acetaldehyde, which forms Schiff base adducts with other macromolecules.
|
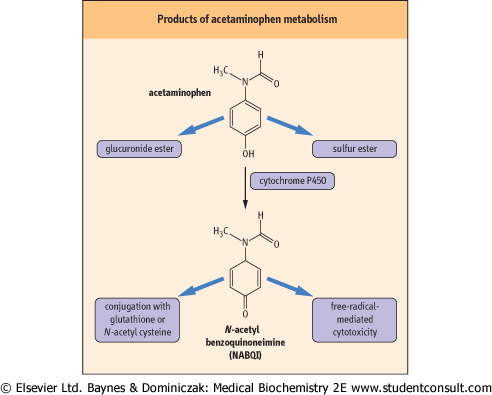
| ACETAMINOPHEN AND HEPATIC FAILURE |
A 22-year-old woman was admitted to hospital in a semiconscious state. She had been found with a suicide note and empty acetaminophen containers. Tests revealed: aspartate aminotransferase (AST) 5500 U/L, alkaline phosphatase (ALP) 125 U/L, bilirubin 70 μmol/L (4.1 mg/dL), prothrombin time 120 s (normal value 10-15 s), creatinine 350 μmol/L (4.0 mg/dL) (normal range 20-80 μmol/L [0.28-0.90 mg/dL]), glucose 2.6 mmol/L (47 mg/dL) (normal range 4.0-6.0 mmol/L [72-109 mg/dL]), and blood pH 7.1. No acetaminophen was found in her plasma. containers. Tests revealed: aspartate aminotransferase (AST) 5500 U/L, alkaline phosphatase (ALP) 125 U/L, bilirubin 70 μmol/L (4.1 mg/dL), prothrombin time 120 s (normal value 10-15 s), creatinine 350 μmol/L (4.0 mg/dL) (normal range 20-80 μmol/L [0.28-0.90 mg/dL]), glucose 2.6 mmol/L (47 mg/dL) (normal range 4.0-6.0 mmol/L [72-109 mg/dL]), and blood pH 7.1. No acetaminophen was found in her plasma. |
| Comment. The patient had acute hepatic failure, most probably caused by acetaminophen poisoning. Blood acetaminophen may be undetectable if the patient first comes to medical attention more than 24 hours after an overdose. The hepatocellular damage worsens over the first 72 hours, but may improve spontaneously after that, as a result of regeneration of hepatocytes. However, in patients with a metabolic acidosis, markedly increased prothrombin times or serum creatinine >300 μmol/L (3.4 mg/dL), mortality is very high, and liver transplantation may be necessary. For reference ranges see Table 28.2. |
|
| The redox potential of the hepatocyte is altered by ethanol oxidation, as a result of the increased ratio of NADH to NAD+.
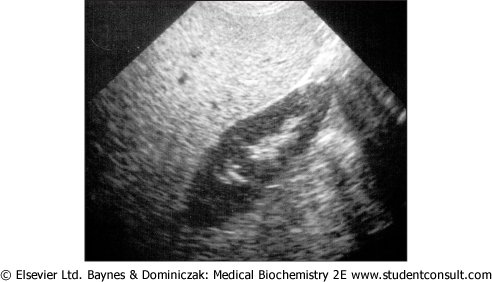
This inhibits the oxidation of lactate to pyruvate - a step that requires NAD+ as a cofactor. There is the potential for lactic acidosis and, because hepatic gluconeogenesis requires pyruvate as a substrate, there is also a risk of hypoglycemia. The likelihood of hypoglycemia is also increased in alcoholics when they fast, as they often have low hepatic stores of glycogen because of poor nutrition. The shift in the NADH/NAD+ ratio also inhibits β-oxidation of fatty acids and promotes triglyceride synthesis; this increases hepatic synthesis of very-low-density lipoprotein, and the excess is deposited in the liver (hepatic steatosis) and secreted into plasma (see clinical boxes on p. 203 and p. 408). Hepatic steatosis is often associated with changes in the serum levels of the transaminase enzymes (see below) which are used by the clinical laboratory to monitor liver disease, but can be readily diagnosed by ultrasonography of the liver when one sees a uniform increased echogenicity (see Fig. 28.9).
|
| The unpleasant symptoms of alcohol intolerance are exploited to reinforce abstinence
|
| page 407 | | | page 408 |
| Figure 28.9 An ultrasound scan of a liver showing steatosis. (courtesy Dr A Bannerjee, Birmingham Heartlands and Solihull NHS Trust, UK). |
| Both alcohol dehydrogenase and ALDH are subject to genetic polymorphisms, which have been investigated as a potential inherited basis of susceptibility to alcoholism and alcoholic liver disease. Possession of the ALDH22 allele, which encodes an enzyme with reduced catalytic activity, leads to increased plasma concentrations of acetaldehyde after the ingestion of
alcohol. This causes the individual to experience unpleasant flushing and sweating, which discourages alcohol abuse. Disulfiram, a drug that inhibits ALDH, also leads to these symptoms when alcohol is taken, and may be given to reinforce abstinence from alcohol. (See also box on p. 242.)
|
|