| Testosterone deficiency may originate from a wide range of disorders of the hypothalamus, pituitary or testes
|
| page 534 |  | | page 535 |
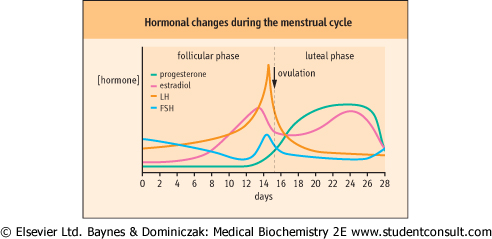
| Figure 37.12 Changes in hormone secretion during the normal menstrual cycle. LH, luteinizing hormone; FSH, follicle stimulating hormone. |
A genetic hypothalamic disorder in children (Kallmann's syndrome) results in deficient GnRH production; affected individuals present with delayed puberty and subnormal FSH, LH, and testosterone . A genetic testicular disorder of the seminiferous tubules (Klinefelter's syndrome, karyotype 47XXY) presents with gynecomastia (abnormal increase in size of the male breast), eunuchoidism, and varying degrees of hypogonadism. Serum FSH is elevated, and LH is usually elevated, but testosterone may be subnormal. The external effects of hypogonadism may be corrected by androgen administration but these patients are sterile. Androgen deficiency in older men may have a specific cause (e.g. a pituitary tumor or mumps orchitis, which is an infection of the testes) or it may be part of the natural aging process. Muscle and fat distribution also change,
and these may be corrected, to some extent, by androgen administration. . A genetic testicular disorder of the seminiferous tubules (Klinefelter's syndrome, karyotype 47XXY) presents with gynecomastia (abnormal increase in size of the male breast), eunuchoidism, and varying degrees of hypogonadism. Serum FSH is elevated, and LH is usually elevated, but testosterone may be subnormal. The external effects of hypogonadism may be corrected by androgen administration but these patients are sterile. Androgen deficiency in older men may have a specific cause (e.g. a pituitary tumor or mumps orchitis, which is an infection of the testes) or it may be part of the natural aging process. Muscle and fat distribution also change,
and these may be corrected, to some extent, by androgen administration.
|
| Androgen excess in males is only seen in precocious puberty
|
| Precocious puberty is a rare condition that may result either from early maturation of the normal hypothalamo-pituitary-gonadal axis, gain-of-function mutations in the LH receptor, or as a result of a tumor that is secreting either androgen or HCG.
|
|