| Arachidonic acid is the precursor of eicosanoids, which encompass prostaglandins, prostacyclins, thromboxanes, and leukotrienes
|
| As a key inflammatory mediator, arachidonic acid (see Chapter 15) is the major precursor of the group of molecules termed eicosanoids, which encompass prostaglandins, prostacyclins, thromboxanes, and leukotrienes. Eicosanoids (Fig. 38.13) act like hormones and signal via G-protein-coupled receptors. They have a wide variety of biological activities, including modulating smooth muscle contraction (vascular tone), platelet aggregation, gastric acid secretion, and salt and water balance, as well as mediating pain and inflammatory responses. Moreover, knockout mice defective in prostaglandin production have shown that prostaglandins have wider roles than was previously realized, being involved in the control of complex processes such as pregnancy, and tumor spread and metastasis in colon cancer (see Chapter 41).
|
| Prostaglandins are synthesized in membranes from arachidonic acid
|
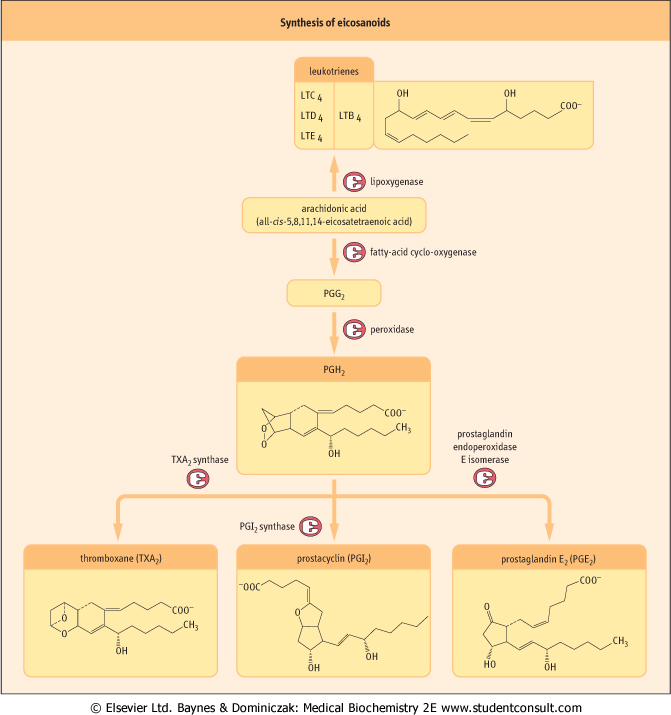
| The first stage in the conversion of arachidonic acid to prostaglandins involves the cyclo-oxygenase component of prostaglandin synthase, which induces the formation of a cyclopentane ring and the introduction of four oxygen atoms to generate the intermediate, prostaglandin G2 (PGG2). PGG2 is then subject to a hydroperoxidase reaction that catalyzes the two-electron reduction of the 15-hydroperoxy group to a 15-hydroxyl group and generates the highly unstable intermediate, PGH2, which can then be converted into other prostaglandins, prostacylin and thromboxane.
|
| page 555 |  | | page 556 |
| Figure 38.13 Synthesis of eicosanoids. Eicosanoids are primarily derived from arachidonic acid. Leukotrienes (LT) are synthesized via a lipoxygenase-dependent pathway, whereas prostaglandins (PG), prostacyclins and thromboxanes (TX) arise from cyclo-oxygenase-dependent routes. |
| page 556 | | | page 557 |
| Figure 38.14 Measurement of cAMP by radioimmunoassay (RIA). Unlabeled cAMP in the patient sample competes with 125I-labeled cAMP assay reagent for binding to pre-immobilized anti-cAMP antibody. After washing, 125I levels are inversely proportional to cAMP levels in the patient sample. Quantitative analysis can be performed by constructing a standard curve. Compare the immunoradiometric sandwich assay for hormones (Fig. 37.2). |
| MCCUNE-ALBRIGHT SYNDROME (INCIDENCE 1 IN 25000) |
| A 3-year-old girl was brought to hospital because her mum had been concerned about apparent breast development over the last 6 months, and a spot of blood on her pants last week. On examination, she had Tanner Stage 3 breast development. On her trunk she had three areas of brown skin pigmentation with ragged edges. |
| Comment. This child is suffering from McCune-Albright Syndrome. She is likely to develop polyostotic fibrous dysplasia, with areas of thinning and sclerosis in her long bones which may fracture. Other endocrinopathies include thyrotoxicosis, GH hypersecretion, Cushing's syndrome (cortisol excess) and hyperparathyroidism. The cause is an activating missense mutation in the gene encoding the Gsα, subunit of the G protein that stimulates cyclic AMP formation. The problem presents following a somatic cell mutation with clinical features dependent on a mosaic distribution of aberrant cells. |
| cAMP RADIO-IMMUNOASSAY (RIA) |
| The action of parathyroid hormone (PTH) on the renal tubule results in release of cAMP into the urine (see Chapter 23). The clinical assessment of cAMP levels is a useful indicator of parathyroid function. 90% of patients with hyperparathyroidism have increased levels of nephrogenous cAMP (urinary cAMP minus plasma cAMP filtered but not reabsorbed in the kidney). Furthermore, infusion with PTH causes a dramatic increase in urinary cAMP concentrations in patients with idiopathic hypoparathyroidism but not type I pseudohypoparathyroidism patients, who have a mutation in Gsα and thus exhibit a defective renal tubular response to PTH, resulting in reduced cAMP secretion. |
| cAMP levels can be analyzed by radio-immunoassay (RIA), which measures the competition for binding to an immobilized cAMP-specific antibody between 125I-labeled cAMP assay reagent and unlabeled cAMP in the patient sample (Fig. 38.14). Quantitative measurement of cAMP levels can be performed using known concentrations of unlabeled cAMP assay reagent to construct a standard curve. |
|
Two distinct isoforms of cyclo-oxygenase, termed COX-1 and COX-2, have been identified. Whereas COX-1 is constitutively expressed, COX-2 is made only in response to
inflammatory mediators such as cytokines. Cyclo-oxygenase inhibitors, the non-steroidal anti-inflammatory drugs (NSAIDs) such as aspirin and ibuprofen, act to reduce inflammation and provide pain relief by blocking this first step in the production of prostaglandins. Although the currently marketed drugs preferentially block COX-1, a number of COX-2-selective drugs are under development because it is believed
that COX-2, being induced under conditions of inflammation, may have a more important role than COX-1 in mediating inflammatory responses. Moreover, the major side effects of blocking COX-1 are bleeding and the inflammation of gastric mucosa, and the use of inhibitors selective for COX-2 may make it possible to target inflammatory activity and thus avoid most of the sequelae associated with the use of COX-1 inhibitors. and ibuprofen, act to reduce inflammation and provide pain relief by blocking this first step in the production of prostaglandins. Although the currently marketed drugs preferentially block COX-1, a number of COX-2-selective drugs are under development because it is believed
that COX-2, being induced under conditions of inflammation, may have a more important role than COX-1 in mediating inflammatory responses. Moreover, the major side effects of blocking COX-1 are bleeding and the inflammation of gastric mucosa, and the use of inhibitors selective for COX-2 may make it possible to target inflammatory activity and thus avoid most of the sequelae associated with the use of COX-1 inhibitors.
|
|