| Digestion and absorption of proteins
|
| The protein load received by the gut is derived from two primary sources: 70-100 g dietary protein and 35-200 g endogenous protein, the latter being either proteins secreted and into the gut (mostly enzymes) or shed as a result of turnover of epithelial cells. Only 1-2 g nitrogen, equivalent to 6-12 g protein, are lost in the feces daily. Thus, the digestion and absorption of protein is extremely efficient.
|
| Proteins are hydrolyzed by peptidases
|
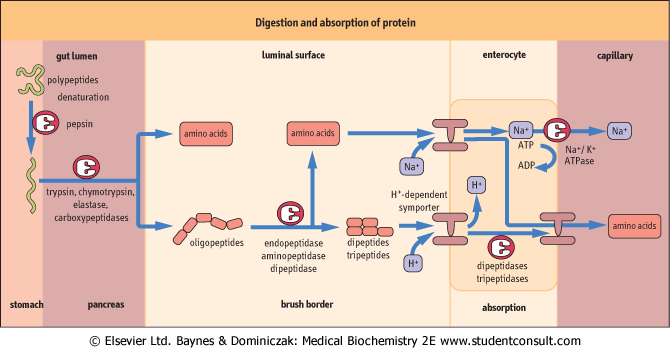
Proteins are broken down by hydrolysis of peptide bonds and hence the enzymes involved are termed 'peptidases'. These enzymes can either cleave internal peptide bonds (endopeptidases) or cleave off one amino acid at a time from either the -COOH or -NH2 terminal of the polypeptide (exopeptidases subclassified into carboxypeptidases and aminopeptidases, respectively). The endopeptidases cut the large polypeptides to smaller oligopeptides, which can be acted upon by the exopeptidases to produce the final products of protein digestion, di- and tripeptides and amino acids , which are then absorbed by the enterocytes. Depending on the source of the peptidases, protein digestion can be divided into gastric, pancreatic and intestinal phases (Fig 9.8 and Table 9.2). The specificity of peptidases is illustrated in Table 9.1. , which are then absorbed by the enterocytes. Depending on the source of the peptidases, protein digestion can be divided into gastric, pancreatic and intestinal phases (Fig 9.8 and Table 9.2). The specificity of peptidases is illustrated in Table 9.1.
|
| Protein digestion begins in the stomach
|
| Different cell types present in the stomach perform different digestive functions. The chief cells secrete pepsinogen, a precursor of a peptidase, pepsin. Pepsinogen is activated to pepsin in the acid environment of the stomach lumen. The parietal cells generate hydrogen ion in the stomach by the action of carbonic anhydrase (see Chapter 23). Hydrogen ion is secreted by the ATP-dependent proton pump located on the luminal membrane of these cells (see Chapter 7, Fig. 7.8). The secretion of the parietal cells is stimulated by the histamine-secreting cells, histamine acting on the H2 receptors on the parietal cells. The G-cells in the stomach secrete the hormone gastrin. Gastrin secretion is stimulated by food entering stomach. |
| Stomach cells also secrete the intrinsic factor (IF) which facilitates the absorption of vitamin B12. Finally stomach cells secrete mucus which is alkaline and protects the stomach lining against the effects of the acid. |
| page 123 |  | | page 124 |
| Figure 9.8 Digestion and absorption of proteins. |
| In the stomach, secreted HCl reduces the pH to 1-2 with consequent denaturation of dietary proteins (Fig. 7.8).
Denaturation makes proteins more accessible to protease activity by the unfolding of the polypeptide chain. In addition, pepsins are secreted by the chief cells of the gastric mucosa. These acid proteases are released as the inactive precursors, pepsinogens A and B, and are activated by either an intramolecular reaction (autoactivation) at a pH below 5 or by active pepsin (autocatalysis). At a pH above 2, the liberated peptide remains bound to pepsin and acts as an inhibitor of pepsin activity. This inhibition is removed by either a decrease in pH below 2 or by further pepsin action. The major products of pepsin digestion of proteins are large peptide fragments and some free amino acids. The gastric protein digests in turn stimulate cholecystokinin release in the duodenum, initiating the release of the main digestive enzymes by the pancreas.
|
| The proteolytic enzymes released from the pancreas are, similarly to the pepsins, released as inactive zymogens: the duodenal enteropeptidase converts trypsinogen to the active trypsin. This enzyme is then capable of autoactivation and and the activation of all other pancreatic zymogens, thus activating chymotrypsin, elastase, and carboxypeptidases A and B. Since the prime role of trypsin is activating other pancreatic enzymes, its activity is controlled within the pancreas and pancreatic ducts by a low molecular weight inhibitory peptide.
|
| ACTIVE TRANSPORT OF AMINO ACIDS INTO INTESTINAL EPITHELIAL CELLS |
| These mechanisms are similar to those described for glucose uptake. At the brush border membrane Na+-dependent symporters (membrane transporters which transport two substances in the same direction - see Chapter 7) for amino acid uptake are linked to ATP-dependent pumping out of Na+ at the contraluminal membrane. A similar H+-dependent symporter is present on the brush-border surface for di- and tri-peptide active transport into the cell. Na+-independent transporters are present on the contraluminal surface, thus allowing the facilitated transport of amino acids to the hepatic portal system. |
From both genetic and transporter studies, at least six specific symporter systems have been identified for the uptake of l-amino acids from the intestinal lumen:
- neutral amino acid symporter for amino acids with short or polar side-chains (Ser, Thr, Ala);
- neutral amino acid symporter for aromatic or hydrophobic side-chains (Phe, Tyr, Met, Val, Leu, Ileu);
- imino acid symporter (Pro, OH-Pro);
- basic amino acid symporter (Lys, Arg, Cys);
- acidic amino acid symporter (Asp, Glu);
- β-amino acid symporter (β-Ala, Tau).
|
| These transport systems are also present in the renal tubules and defects in their constituent protein structure can lead to disease (e.g. Hartnup disease). Pathologies of similar mechanism can thus be produced in both the kidney and intestine. |
| page 124 | | | page 125 |
| A 15-year-old African-American boy came across to the UK on an exchange visit for 2 months. After 2 weeks in the UK, he complained of abdominal discomfort, a feeling of being bloated, increased passage of urine and, more recently, the development of diarrhoea. His only change in diet noted at the time was the introduction of milk into his diet. He had developed a considerable liking for milk and was consuming 1-2 large cartons per day. A lactose tolerance test was performed, whereby the young man was given 50 g lactose in an aqueous vehicle to drink. Plasma glucose levels did not rise by more than 1 mmol/L (18 mg/dL) over the next 2 hours, with sampling at 30-minute intervals. A diagnosis of lactose intolerance was made. |
| Comment. Lactose intolerance is a physiologic change resulting from acquired lactase deficiency. Lactase activity decreases with increasing age in children but the extent of the decline in activity genetically determined and demonstrates ethnic variation. Lactase deficiency in the adult black population varies from 45-95%. If symptoms of malabsorption occur after the introduction of milk to adult diets, the diagnosis of acquired lactase deficiency should be considered. A diagnosis is made by challenging the small bowel with lactose and monitoring the rise in plasma glucose. An increase of more than 1.7 mmol/L (30 mg/dL) is considered normal. A rise of less than 1.1 mmol/L (20 mg/dL) is diagnostic of lactase deficiency. A rise of 1.1-1.7 mmol/L (20-30 mg/dL) is inconclusive. |
| Pancreatic proteases have different substrate specificity with respect to peptide bond cleavage
|
| Trypsin cleaves proteins at lysine and arginine residues, chymotrypsin at aromatic amino acids and elastase at smaller hydrophobic amino acids. The combined effect of these pancreatic enzymes is to produce an abundance of free amino acids and small molecular weight peptides of two to eight residues in length.
|
| In association with protease secretion, the pancreas also produces copious amounts of sodium bicarbonate (NaHCO3). This results in the neutralization of the acid contents of the stomach, promoting pancreatic alkaline protease activity.
|
| Endopeptidases, dipeptidases and aminopeptidases complete the digestion of proteins
|
| A 22-year-old man presented with a history of weight loss, diarrhea, abdominal bloating and anemia. He described his stools as pale and bulky. Laboratory features included hemoglobin of 90 g/L (9 g/dL) (reference range 130-180 g/L; 13-18 g/dL). Biopsy of his small bowel demonstrated flattening of the mucosal surface, villous atrophy and disappearance of microvilli. A diagnosis of gluten-induced enteropathy or coeliac disease was made. All wheat products were removed from the patient's diet and the symptoms resolved. |
| Comment. Coeliac disease is an autoimmune condition characterized by malabsorption and specific diagnostic features exhibited by the intestinal mucosa. Since the absorptive surface is markedly reduced, the resulting indigestion/malabsorption is severe. The histologic changes are due to the interaction of gluten, the principal protein of wheat, with the epithelium. There is evidence to suggest that the deficit is located within the mucosal cells of the intestine and permits polypeptides, resulting from peptic and tryptic digestion of gluten, not only to exert local harmful effects within the intestine but also to be absorbed and to induce an antibody response. Circulating antibodies to wheat gluten and its fractions are frequently present in cases of coeliac disease. The use of sensitive and specific serological screening tests, such as endomysial antibodies of IgA subclass has shown that coeliac disease is under-diagnosed, especially in patients with unexplained anaemia. |
| The final digestion of oligo- and dipeptides is dependent on membrane-bound small intestinal endopeptidases, dipeptidases, and aminopeptidases. The end-products of this surface enzyme activity are free amino acids, and di- and tripeptides which can then be absorbed across the enterocyte membrane
by specific carrier-mediated transport. Di- and tripeptides are further hydrolyzed to their constituent amino acids inside the enterocyte. The final step is the transfer of the free amino acids across the contraluminal plasma membrane into the portal system.
|
| Certain carbohydrates and proteins cannot be properly digested by some individuals and lead to the development of disease. The commonest of these is lactose intolerance and gluten (wheat protein) sensitivity, the latter also known as coeliac disease (see the two boxes on this page). Elimination of these foods from the diet is, in essence, the treatment for these particular pathologies.
|
|