| CARDIOVASCULAR RISK AND ITS ASSESSMENT
|
| Plasma concentrations of lipoproteins are one of the important factors in the assessment of the cardiovascular risk of an individual (a probability that that person will suffer from heart attack or stroke in the future). However, there are also other, non-lipid cardiovascular risk factors, and they are listed in Table 17.5.
|
| page 240 |  | | page 241 |
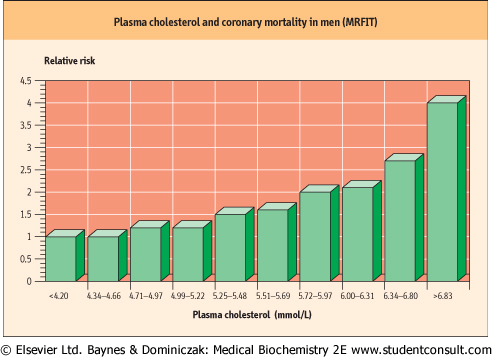
| Figure 17.11 Plasma cholesterol and coronary mortality in men. Total cholesterol concentration in plasma in relation to the number of deaths from heart disease in a population. Note: converting plasma lipid values into SI units: cholesterol: to convert mg/dL into mmol/L, mutliply by 0.02586; triglycerides: to convert mg/dL into mmol/L, multiply by 0.01129. The data are from the Multiple Risk Factor Intervention Trial (MRFIT). Stammler et al. JAMA 1986;256:2823. |
|
Table 17-5.
Cardiovascular risk factors and their management. |
| Body_ID: None |
| Cardiovascular risk factors and their management |
| Body_ID: T017005.50 |
| Risk factor | Comment | Remedy |
| Body_ID: T017005.100 |
| Male sex | the difference in cardiovascular risk between sexes equalizes in postmenopausal women | |
| Body_ID: T017005.150 |
| Age | | |
| Body_ID: T017005.200 |
| Smoking | | smoking cessation |
| Body_ID: T017005.250 |
| High plasma cholesterol (high LDL-cholesterol) | 2-3% decrease in risk for 1% decrease of total plasma cholesterol | diet low in saturated fats and, where appropriate, cholesterol-lowering drugs |
| Body_ID: T017005.300 |
| Low plasma HDL | | smoking cessation, regular exercise |
| Body_ID: T017005.350 |
| Hypertension | major risk factor for stroke and a risk factor for CHD | control blood pressure: diet and drugs |
| Body_ID: T017005.400 |
| Obesity | | weight reduction |
| Body_ID: T017005.450 |
| Sedentary lifestyle | | regular moderate exercise |
| Body_ID: T017005.500 |
| Diabetes | cardiovascular disease is the main cause of death in diabetes | diet and drugs (insulin in type 1 diabetes). Lipid-lowering if dyslipidemia present |
| Body_ID: T017005.550 |
|
| Body_ID: T017005.600 |
Plasma lipids are not the only factors that determine the risk of cardiovascular disease. This table lists the most important cardiovascular risk factors and the risk-reducing strategies used in cardiovascular prevention. You will find more on dietary aspects of cardiovascular prevention in Chapter 21.
|
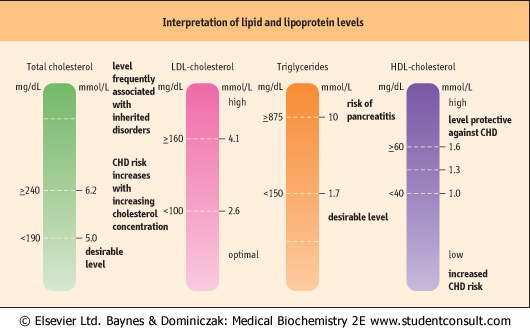
| As far as lipids are concerned, the risk of cardiovascular disease is related to plasma concentrations of total cholesterol (Fig. 17.11), LDL-cholesterol, HDL-cholesterol, and triacylglycerols (triglycerides) The inclusion of triglycerides had been disputed for a long time, and some risk factor lists do not include them to this date. However, recent research made it quite clear that they contribute to risk (Fig. 17.10). The risk increases when the total cholesterol level is above 5.2 mmol/L (200 mg/dL). According to the recommendations of the U.S. National Cholesterol Education Program, the desirable level of total cholesterol is that below 5.2 mmol/L (200 mg/dL) and the optimal level of LDL-cholesterol is below 2.6 mmol/L (100 mg/dL). In contrast to LDL, the relationship between the HDL concentration and cardiovascular risk is inverse: it is the low concentration of HDL which signifies increased risk. The undesirably low concentration of HDL-cholesterol is below 1 mmol/L (40 g/dL) but a concentration above 1.6 mmol/L (60 mg/dL) is regarded as providing some protection against
coronary disease. Clinical interpretation of the fasting lipid profile is summarized in Figure 17.11.
|
| One should remember that the risk associated with lipid concentration can be modified by other factors, such as increased concentration of Lp(a), plasma homocysteine, fibrinogen, or C-reactive protein (CRP; see below). In fact, about 50% of persons who suffer from myocardial infarction have 'average' lipid concentrations. Thus, the search continues for new markers that would more precisely define individual cardiovascular risk. The measurement of substances associated with the inflammatory response, such as small increases in plasma CRP concentration, seem to fulfill this role particularly well.
|
| page 241 | | | page 242 |
| Figure 17.12 The interpretation of cholesterol, triglyceride, and HDL-cholesterol measurements. To convert plasma lipid values into conventional units: total cholesterol, LDL-cholesterol, and HDL-cholesterol: to convert mmol/L into mg/dL: multiply by 38.67; triglycerides: to convert mmol/L into mg/dL, multiply by 87.5. CHD, coronary heart disease. |
| LIFESTYLE CHANGE IMPROVES PLASMA LIPID PROFILE |
| A 57-year-old man was referred to the lipid clinic because of hypertriglyceridemia (high triacylglycerol concentration). His triglycerides were 6 mmol/L (545 mg/dL), cholesterol was 5 mmol/L (192 mg/dL), and HDL was 1 mmol/L (39 mg/dL). He was obese, took 30 units of alcohol per week, and led a sedentary lifestyle. |
| After a hesitant start he eventually managed to lose 7 kg of weight over 6 months, cut drinking to below 20 units per week, and started to exercise regularly. Twelve months later, his triglycerides were 2.5 mmol/L (227 mg/dL), cholesterol 4.8 mmol/L (186 mg/dL), and HDL 1.2 mmol/L (46 mg/dL). |
| Comment. Lifestyle change may result in appreciable improvements in the lipid profile. To achieve this, the individuals must be committed to changing lifestyle and to maintaining the change over a prolonged period of time. In practice this is often difficult. |
| Note: 1 unit of alcohol is a one measure (60 mL) of liquor, a one glass (170 mL) of wine, or a half-pint (300 mL) of beer. |
| The risk of an atherosclerotic event such as myocardial infarction or stroke, can be decreased by eliminating risk factors through diet, exercise, smoking cessation, control of
high blood pressure, and by lowering undesirably high plasma lipoprotein concentrations (Table 17.5).
|
The concentration of plasma LDL (and consequently total plasma cholesterol) can decrease when a person follows a low-cholesterol diet. In addition, there are several drugs that lower plasma cholesterol concentration either by inhibiting intracellular cholesterol synthesis (HMG-CoA reductase inhibitors known as statins, which primarily lower plasma cholesterol), by stimulating LPL, decreasing triacylglycerol concentration, and increasing HDL (derivatives of fibric acid, fibrates), or by preventing cholesterol absorption in the intestine (bile acid binding resins, now relatively rarely used, and ezetimibe , an inhibitor of intestinal cholesterol transporter). , an inhibitor of intestinal cholesterol transporter).
|
| In animals, antioxidants such as probucol, vitamin E, or butylated hydroxytoluene inhibit atherosclerotic changes. β-carotene and α-tocopherol protect LDL against oxidation in vitro and treatment with antioxidants increases the resistance of LDL to oxidation. Epidemiologic studies have shown that those who take antioxidants such as vitamin E and C or β-carotene have cardiovascular disease less often. However, the puzzling finding is that the prospective clinical trials of antioxidant treatment have failed to confirm their preventive benefit. One tentative explanation for this is that it is the natural antioxidants (such as these contained in fruits) or their combinations, rather than single pure substances which are protective.
|
| The most important, however, is this: since arteriosclerosis is a multifactorial process, the effective cardiovascular prevention needs to involve a comprehensive approach which combines lifestyle modification (smoking cessation, diet and exercise) with appropriate treatment of dyslipidemia, hypertension and diabetes.
|
| page 242 | | | page 243 |
| THE PRESENCE OF XANTHELASMA DOES NOT NECESSARILY SIGNIFY A LIPID DISORDER |
| A 28-year-old lady developed unsightly yellow marks around both eyes, so-called xanthelasma but otherwise she was asymptomatic. Her cholesterol was 5.0 mmol/L (192 mg/dL), triglycerides 0.7 mmol/L (64 mg/dL), and her HDL-cholesterol was 1.4 mmol/L (53 mg/dL). There was no family history of early coronary disease. |
| Comment. Xanthelasma may occur in individuals with completely normal lipid levels. On the other hand, lipid deposits in tendons (tendon xanthomata) are always diagnostic of familial lipid disorder. The patient was reassured and referred for cosmetic surgery. |
|