| WATER REABSORPTION IN THE DISTAL TUBULE AND THE COLLECTING DUCT
|
| Aquaporins are a family of membrane channel proteins which enable rapid transport of water through biological membranes.
|
| Figure 22.16 Aquaporin water channel. Aquaporin-1 is a multisubunit water channel with a glycan unit attached to one of the subunits (A). Each of the two monomers has two tandem repeat structures each consisting of three membrane-spanning regions (B) and connecting loops containing asn-pro-ala (NPA) sequences embedded in the membrane bilayer. |
Aquaporin O (AQPOP) gene is expressed in lens cells and the mutations of its gene are associated with congenital cataracts. AQP1 is expressed in erythrocytes, renal proximal tubular cells, and in the capillary endothelium. AQP2 is principally expressed in the renal collecting ducts. Mutations in AQP2 gene and in the vasopressin receptor gene lead to different
types of the so-called nephrogenic diabetes insipidus, a condition associated with passing large amounts of urine and dehydration (Fig. 22.16). receptor gene lead to different
types of the so-called nephrogenic diabetes insipidus, a condition associated with passing large amounts of urine and dehydration (Fig. 22.16).
|
| Vasopressin (antidiuretic hormone, ADH) controls water reabsorption in the collecting ducts of the kidney
|
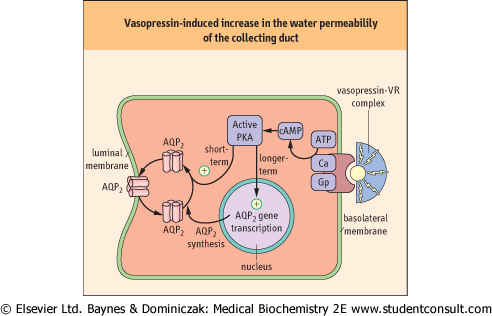
| Vasopressin is synthesized in the supraoptic and paraventricular nuclei of the hypothalamus and transported along axons to the posterior pituitary where it is stored before being further processed and released. The binding of vasopressin to its receptor located on the membranes of tubular cells in the collecting ducts leads to the synthesis of a variety of proteins, including aquaporin-2, which facilitates passage of water through the membrane (Fig. 22.17). The action of vasopressin determines the final volume and concentration of the urine (see Fig. 22.18).
|
| page 328 |  | | page 329 |
| Figure 22.17 Vasopressin-induced increase in the water permeability of the collecting duct. Aquaporins regulate transport of water across cell membrane. Aquaporin-2 (AQP2) water channel is regulated by vasopressin. Vaspopressin binds to its receptor (VR) and through the activation of G-protein stimulates the production of cAMP which activates protein kinase A (PKA) activity. PKA phosphorylates cytoplasmic AQP2 and induces its translocation to the cell membrane, increasing capacity for water transport. Vasopressin also regulates the expression of the AQP2 gene. |
| POOR FLUID INTAKE LEADS TO DEHYDRATION |
| An 80-year-old man had been admitted to hospital after a prolonged period on the floor at home as a result of an acute stroke. He had poor tissue turgor, dry mouth, tachycardia and hypotension. Serum measurements revealed: sodium 150 mmol/L, potassium 5.2 mmol/L, bicarbonate 35 mmol/L, creatinine 110 μmol/L (1.13 mg/dL), and urea 19 mmol/L (90.3 mg/dL). |
Reference values are:
- sodium: 135-145 mmol/L
- potassium: 3.5-.0 mmol/L
- bicarbonate: 20-25 mmol/L
- creatinine: 20-80 μmol/L (0.28-0.90 mg/dL)
- urea: 2.5-6.5 mmol/L (16.2-39mg/dL)
|
| Comment. This patient presents with dehydration, indicated by the high sodium and urea values. He was treated with intravenous fluid predominantly in the form of 5% dextrose to replace the water deficit. The water deficit can be calculated from tables which give estimates of total body water based on age and leanness. In the adult, total body water is usually about 60% of body weight. |
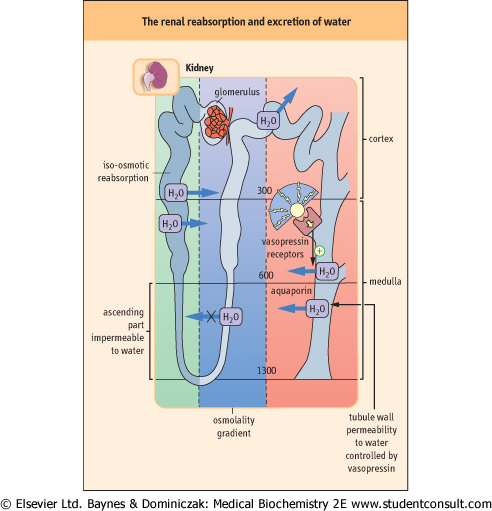
| Figure 22.18 The renal reabsorption and excretion of water. The permeability of the tubular walls to water differs along the nephron. About 80% of filtered water is reabsorbed in the proximal tubule, by iso-osmotic reabsorption. The ascending loop of Henle is impermeable to water; sodium is reabsorbed there, creating high osmolality in the medulla. In the collecting duct, vasopressin controls the reabsorption of water through aquaporin water channels. |
| ENDOCRINE CAUSES OF HYPERTENSION |
| Disorders of aldosterone secretion |
| Hyperaldosteronism is a common finding in hypertension. Primary hyperaldosteronism occurs as a result of abnormal adrenal activity and is rare. It may be a result of a single adrenal tumor, adenoma (Conn's syndrome). The more common secondary hyperaldosteronism is due to an increased secretion of renin. Pheochromocytomas are catecholamine-secreting tumors that cause hypertension in about 0.1% of hypertensive patients. It is important to correctly diagnose pheochromocytoma, because it can be surgically removed (see Chapter 40, clinical box on p. 576). |
| page 329 | | | page 330 |
| ARTERIAL HYPERTENSION IS A COMMON DISEASE |
| Hypertension is inappropriately increased arterial blood pressure above the desirable level of systolic blood pressure 140 mmHg and diastolic pressure 90 mmHg (normal below 140/90 mmHg, optimal below 120/80 mmHg). According to the World Health Organization, up to 20% of the population of the developed world may suffer from the condition. Hypertension causes one in every eight deaths worldwide. Traditionally, arterial hypertension has been classified as 'essential' (primary) or 'secondary'. A cause of essential hypertension has not yet been identified, although it is known to involve multiple genetic and environmental factors including neural, endocrine, and metabolic components. Hypertension is associated with an increased risk of stroke and myocardial infarction. A range of drugs is used in the modern treatment of hypertension. These include diuretics such as bendrofluazide, the drugs blocking adrenoreceptors, the inhibitors of the angiotensin converting enzyme and the antagonists of angiotensin receptors. |
|