| Excluding genetic defects, childhood disease and accidents, humans survive until about age 50 with limited maintenance requirements or risk of death, then we become increasingly frail and our death rate increases, reaching a maximum at about age 76. Our lifespan is affected by our genetics and our environmental exposure, and our death is usually attributable to failure of a critical system (cardiovascular, renal, pulmonary, etc.). The capacity of these inter-dependent physiological systems usually declines as a linear function of age, leading to an exponential increase in our age-specific death rate (Fig. 42.1). Historically, improvements in health care and environment have resulted in rectangularization of the survival curve - the mean lifespan is increased without an increase in the maximum lifespan potential.
|
| THE HAYFLICK LIMIT - REPLICATIVE SENESCENCE |
| Differentiated cells from higher animals undergo only a limited number of cell divisions (population doublings) in tissue culture, unless they become transformed or are infected with certain viruses. The number of potential cell divisions is greater in longer-lived animals, suggesting a relationship between cell division potential and longevity. Human neonatal fibroblasts will divide about 60 times, then enter a non-dividing state. Cells from younger donors have greater replicative capacity, a greater number of cell divisions in cell culture, but with each generation, the number of dividing cells decreases. This limited doubling capacity, described by Dr Leonard Hayflick, is known as the Hayflick limit. The relevance of the Hayflick limit to human aging is still debated - certainly human cells retain some replicative capacity, even at advanced age, and major tissues, such as muscle and nerve, are largely post-mitotic, i.e. not actively dividing. However, changes in the metabolism and morphology of senescent cells, their responsiveness to hormones and their synthetic and degradative capacity, e.g. in the immunological and endothelial systems, may affect our adaptability and susceptibility to age-related diseases, placing limits on our lifespan. |
| page 599 |  | | page 600 |
| Figure 42.1 Survival curve and death rate. (A) Mean lifespan is defined as the age at which 50% of a population survives (or has died). The negative slope of the survival curve reaches a maximum at the mean lifespan of a species. (B) The death rate reaches a maximum at the mean lifespan. (C) The age-specific death rate, defined as the number of deaths per time at a given age, e.g. deaths per 100 000 persons of a specific age per year, increases exponentially with age. The lifespan or maximum lifespan potential (MLSP) is defined as the maximum age attainable by a member of the population, which is 120 years for humans. |
|
Table 42-1.
Decline in biochemical and physiological systems with age. |
| Body_ID: None |
| Changes in biochemistry and physiology during aging |
| Body_ID: T042001.50 |
| Biochemical | Physiological |
| Body_ID: T042001.100 |
| Basal metabolic rate | Lung expansion volume |
| Body_ID: T042001.150 |
| Protein turnover | Renal filtration capacity (glomerular) |
| Body_ID: T042001.200 |
Glucose tolerance tolerance | Renal concentration capacity (tubular) |
| Body_ID: T042001.250 |
| Reproductive capacity | Cardiovascular performance |
| Body_ID: T042001.300 |
| Telomere shortening | Musculoskeletal system |
| Body_ID: T042001.350 |
| Oxidative phosphorylation | Nerve conduction velocity |
| Body_ID: T042001.400 |
| | Endocrine and exocrine systems |
| Body_ID: T042001.450 |
| | Reproductive and immunological systems |
| Body_ID: T042001.500 |
| | Sensory systems (vision, audition) |
| Body_ID: T042001.550 |
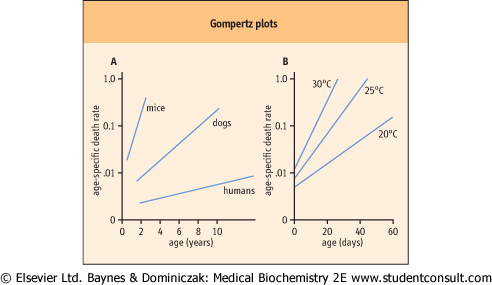
| Figure 42.2 Gompertz plots for humans and other species. (A) Humans and other vertebrates; (B) Flies raised at various temperatures (adapted from work of Prof RS Sohal). |
|